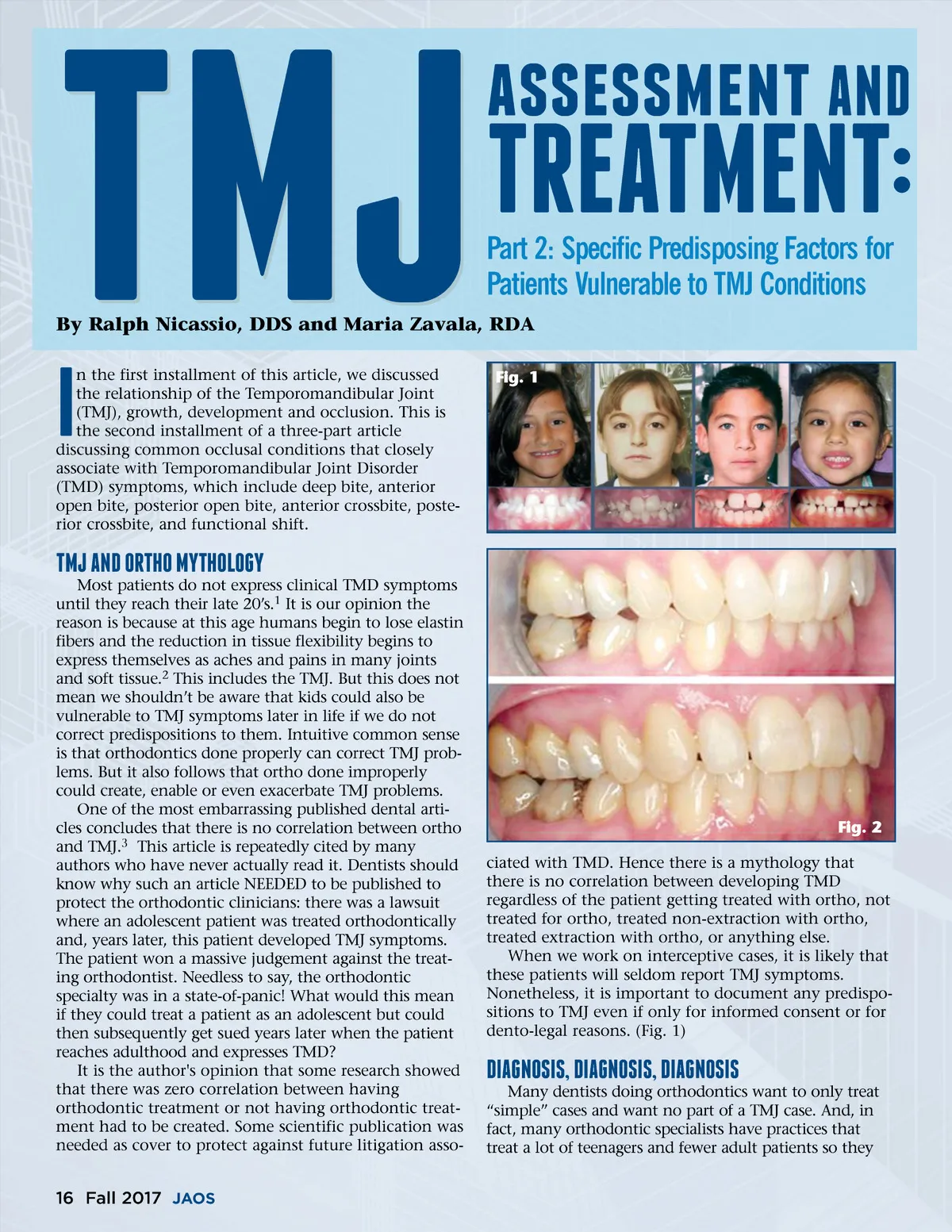
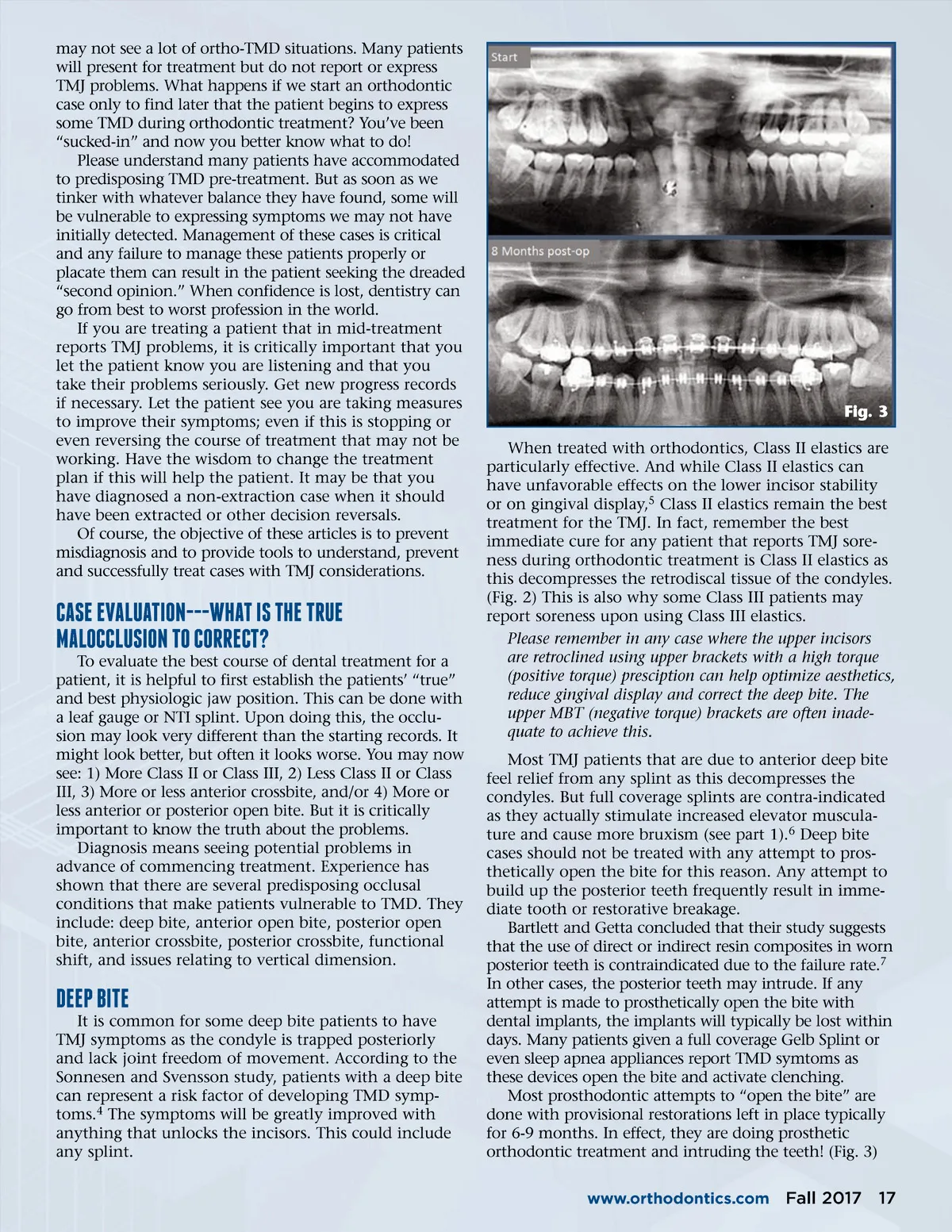
may not see a lot of ortho-TMD situations. Many patients will present for treatment but do not report or express TMJ problems. What happens if we start an orthodontic case only to find later that the patient begins to express some TMD during orthodontic treatment? You’ve been “sucked-in” and now you better know what to do! Please understand many patients have accommodated to predisposing TMD pre-treatment. But as soon as we tinker with whatever balance they have found, some will be vulnerable to expressing symptoms we may not have initially detected. Management of these cases is critical and any failure to manage these patients properly or placate them can result in the patient seeking the dreaded “second opinion.” When confidence is lost, dentistry can go from best to worst profession in the world. If you are treating a patient that in mid-treatment reports TMJ problems, it is critically important that you let the patient know you are listening and that you take their problems seriously. Get new progress records if necessary. Let the patient see you are taking measures to improve their symptoms; even if this is stopping or even reversing the course of treatment that may not be working. Have the wisdom to change the treatment plan if this will help the patient. It may be that you have diagnosed a non-extraction case when it should have been extracted or other decision reversals. Of course, the objective of these articles is to prevent misdiagnosis and to provide tools to understand, prevent and successfully treat cases with TMJ considerations. Fig. 3 When treated with orthodontics, Class II elastics are particularly effective. And while Class II elastics can have unfavorable effects on the lower incisor stability or on gingival display, 5 Class II elastics remain the best treatment for the TMJ. In fact, remember the best immediate cure for any patient that reports TMJ sore-ness during orthodontic treatment is Class II elastics as this decompresses the retrodiscal tissue of the condyles. (Fig. 2) This is also why some Class III patients may report soreness upon using Class III elastics. Please remember in any case where the upper incisors are retroclined using upper brackets with a high torque (positive torque) presciption can help optimize aesthetics, reduce gingival display and correct the deep bite. The upper MBT (negative torque) brackets are often inade-quate to achieve this. Most TMJ patients that are due to anterior deep bite feel relief from any splint as this decompresses the condyles. But full coverage splints are contra-indicated as they actually stimulate increased elevator muscula-ture and cause more bruxism (see part 1). 6 Deep bite cases should not be treated with any attempt to pros-thetically open the bite for this reason. Any attempt to build up the posterior teeth frequently result in imme-diate tooth or restorative breakage. Bartlett and Getta concluded that their study suggests that the use of direct or indirect resin composites in worn posterior teeth is contraindicated due to the failure rate. 7 In other cases, the posterior teeth may intrude. If any attempt is made to prosthetically open the bite with dental implants, the implants will typically be lost within days. Many patients given a full coverage Gelb Splint or even sleep apnea appliances report TMD symtoms as these devices open the bite and activate clenching. Most prosthodontic attempts to “open the bite” are done with provisional restorations left in place typically for 6-9 months. In effect, they are doing prosthetic orthodontic treatment and intruding the teeth! (Fig. 3) www.orthodontics.com CAsE EvAluATION---WhAT Is ThE TRuE MAlOCClusION TO CORRECT? To evaluate the best course of dental treatment for a patient, it is helpful to first establish the patients’ “true” and best physiologic jaw position. This can be done with a leaf gauge or NTI splint. Upon doing this, the occlu-sion may look very different than the starting records. It might look better, but often it looks worse. You may now see: 1) More Class II or Class III, 2) Less Class II or Class III, 3) More or less anterior crossbite, and/or 4) More or less anterior or posterior open bite. But it is critically important to know the truth about the problems. Diagnosis means seeing potential problems in advance of commencing treatment. Experience has shown that there are several predisposing occlusal conditions that make patients vulnerable to TMD. They include: deep bite, anterior open bite, posterior open bite, anterior crossbite, posterior crossbite, functional shift, and issues relating to vertical dimension. DEEp BITE It is common for some deep bite patients to have TMJ symptoms as the condyle is trapped posteriorly and lack joint freedom of movement. According to the Sonnesen and Svensson study, patients with a deep bite can represent a risk factor of developing TMD symp-toms. 4 The symptoms will be greatly improved with anything that unlocks the incisors. This could include any splint. Fall 2017 17
Journal of the American Orthodontic Society Fall 2017: Page 17