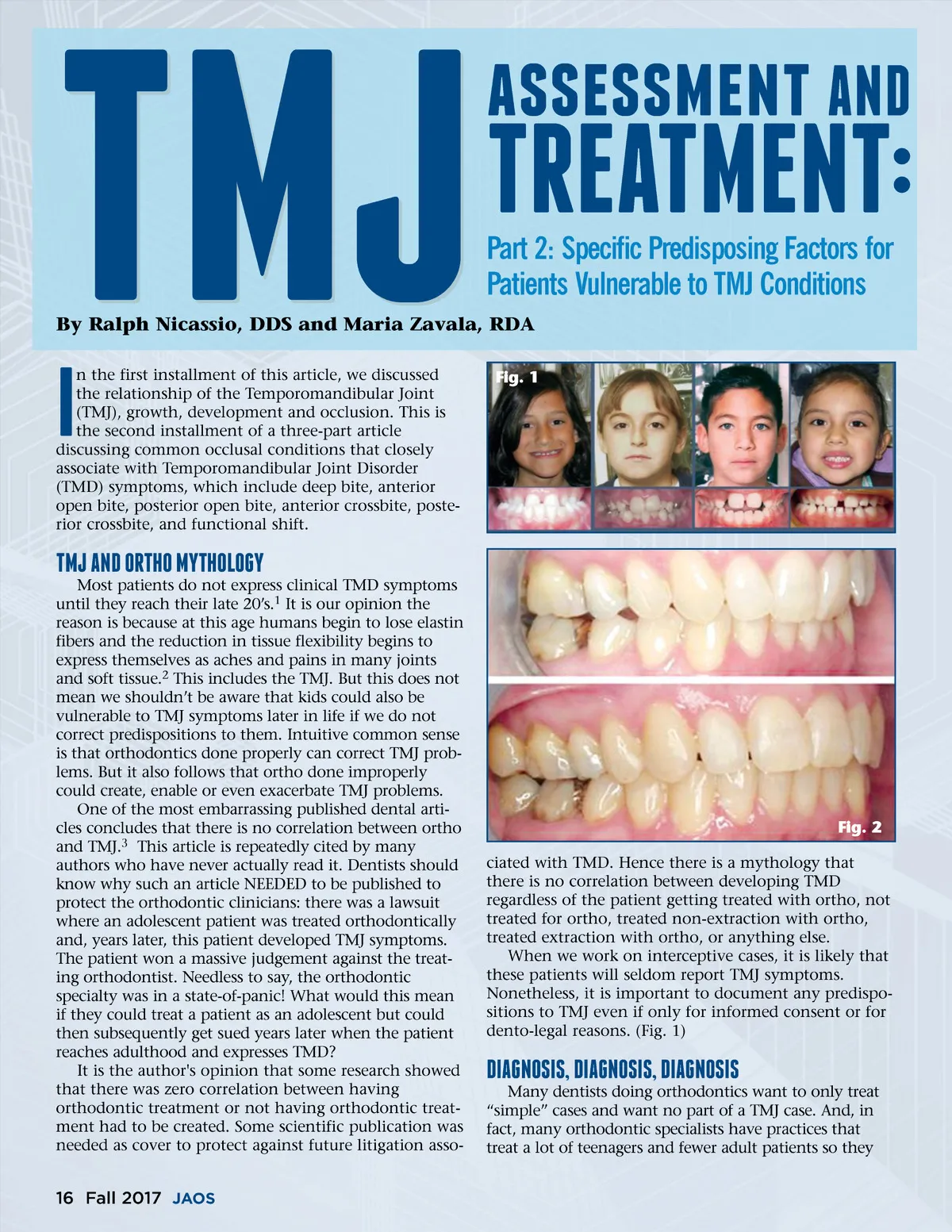
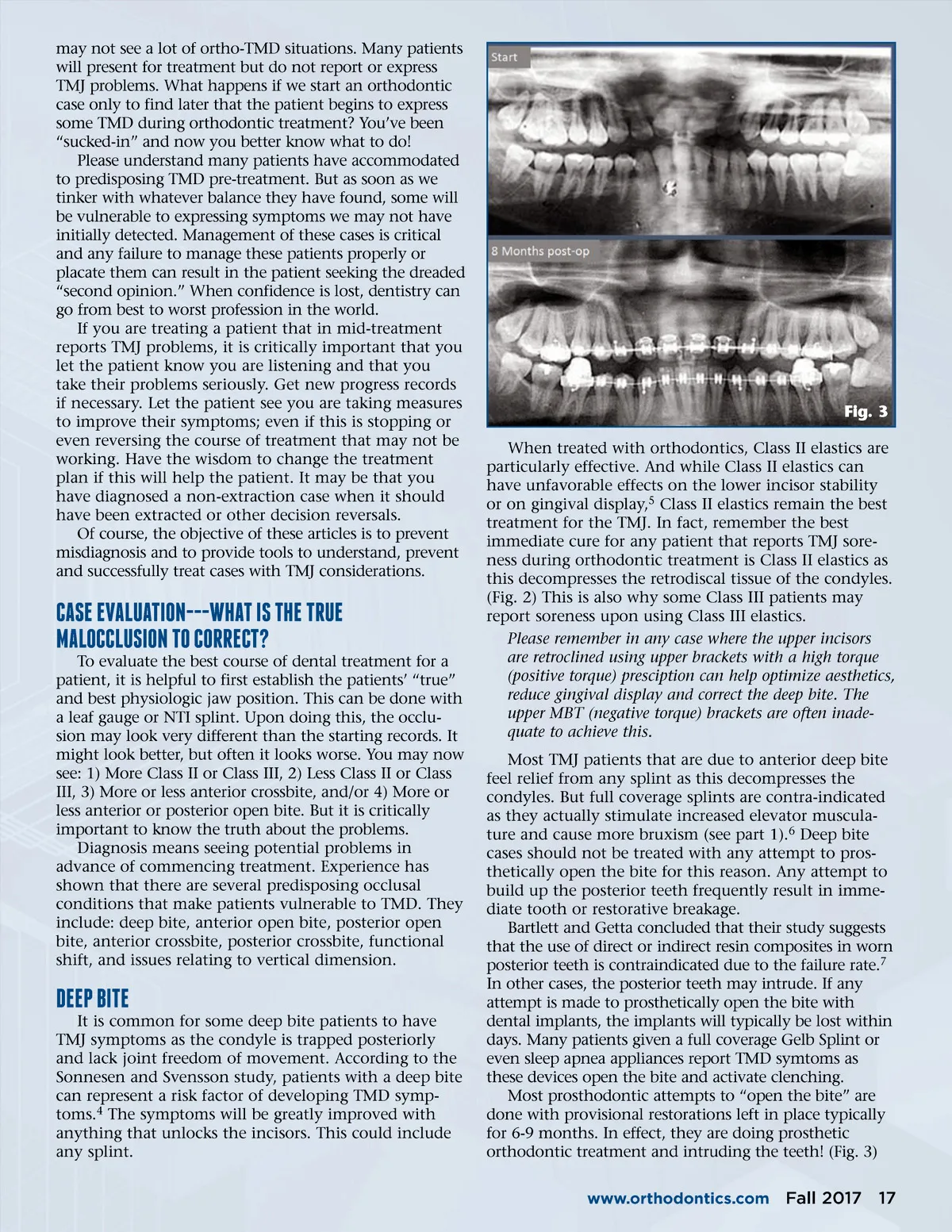
TMJ n the first installment of this article, we discussed the relationship of the Temporomandibular Joint (TMJ), growth, development and occlusion. This is the second installment of a three-part article discussing common occlusal conditions that closely associate with Temporomandibular Joint Disorder (TMD) symptoms, which include deep bite, anterior open bite, posterior open bite, anterior crossbite, poste-rior crossbite, and functional shift. assessment AND Part 2: Specific Predisposing Factors for Patients Vulnerable to TMJ Conditions Fig. 1 TREATMENT: By Ralph Nicassio, DDS and Maria Zavala, RDA I TMJ AND ORThO MyThOlOgy Most patients do not express clinical TMD symptoms until they reach their late 20’s. 1 It is our opinion the reason is because at this age humans begin to lose elastin fibers and the reduction in tissue flexibility begins to express themselves as aches and pains in many joints and soft tissue. 2 This includes the TMJ. But this does not mean we shouldn’t be aware that kids could also be vulnerable to TMJ symptoms later in life if we do not correct predispositions to them. Intuitive common sense is that orthodontics done properly can correct TMJ prob-lems. But it also follows that ortho done improperly could create, enable or even exacerbate TMJ problems. One of the most embarrassing published dental arti-cles concludes that there is no correlation between ortho and TMJ. 3 This article is repeatedly cited by many authors who have never actually read it. Dentists should know why such an article NEEDED to be published to protect the orthodontic clinicians: there was a lawsuit where an adolescent patient was treated orthodontically and, years later, this patient developed TMJ symptoms. The patient won a massive judgement against the treat-ing orthodontist. Needless to say, the orthodontic specialty was in a state-of-panic! What would this mean if they could treat a patient as an adolescent but could then subsequently get sued years later when the patient reaches adulthood and expresses TMD? It is the author's opinion that some research showed that there was zero correlation between having orthodontic treatment or not having orthodontic treat-ment had to be created. Some scientific publication was needed as cover to protect against future litigation asso-Fig. 2 ciated with TMD. Hence there is a mythology that there is no correlation between developing TMD regardless of the patient getting treated with ortho, not treated for ortho, treated non-extraction with ortho, treated extraction with ortho, or anything else. When we work on interceptive cases, it is likely that these patients will seldom report TMJ symptoms. Nonetheless, it is important to document any predispo-sitions to TMJ even if only for informed consent or for dento-legal reasons. (Fig. 1) DIAgNOsIs, DIAgNOsIs, DIAgNOsIs Many dentists doing orthodontics want to only treat “simple” cases and want no part of a TMJ case. And, in fact, many orthodontic specialists have practices that treat a lot of teenagers and fewer adult patients so they 16 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 16