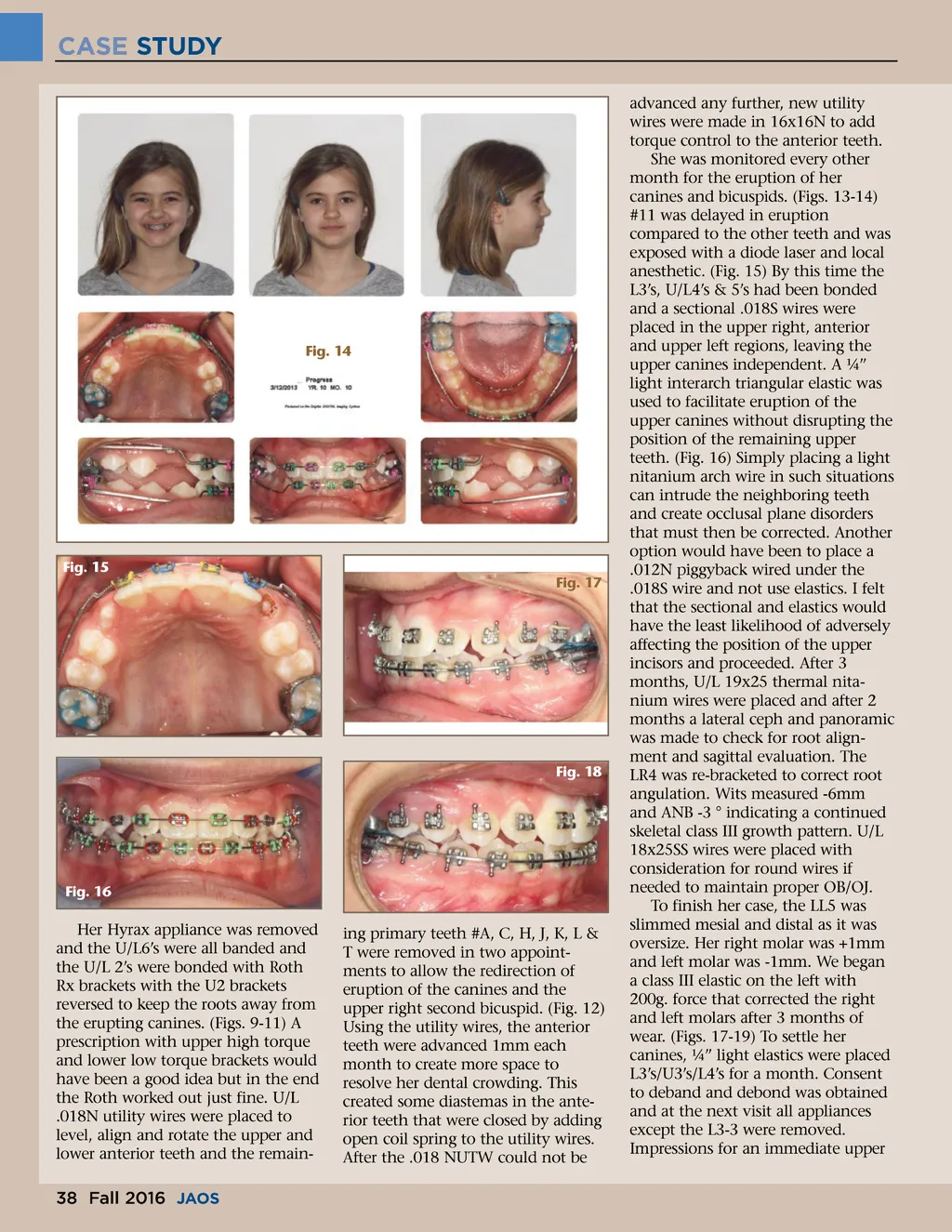
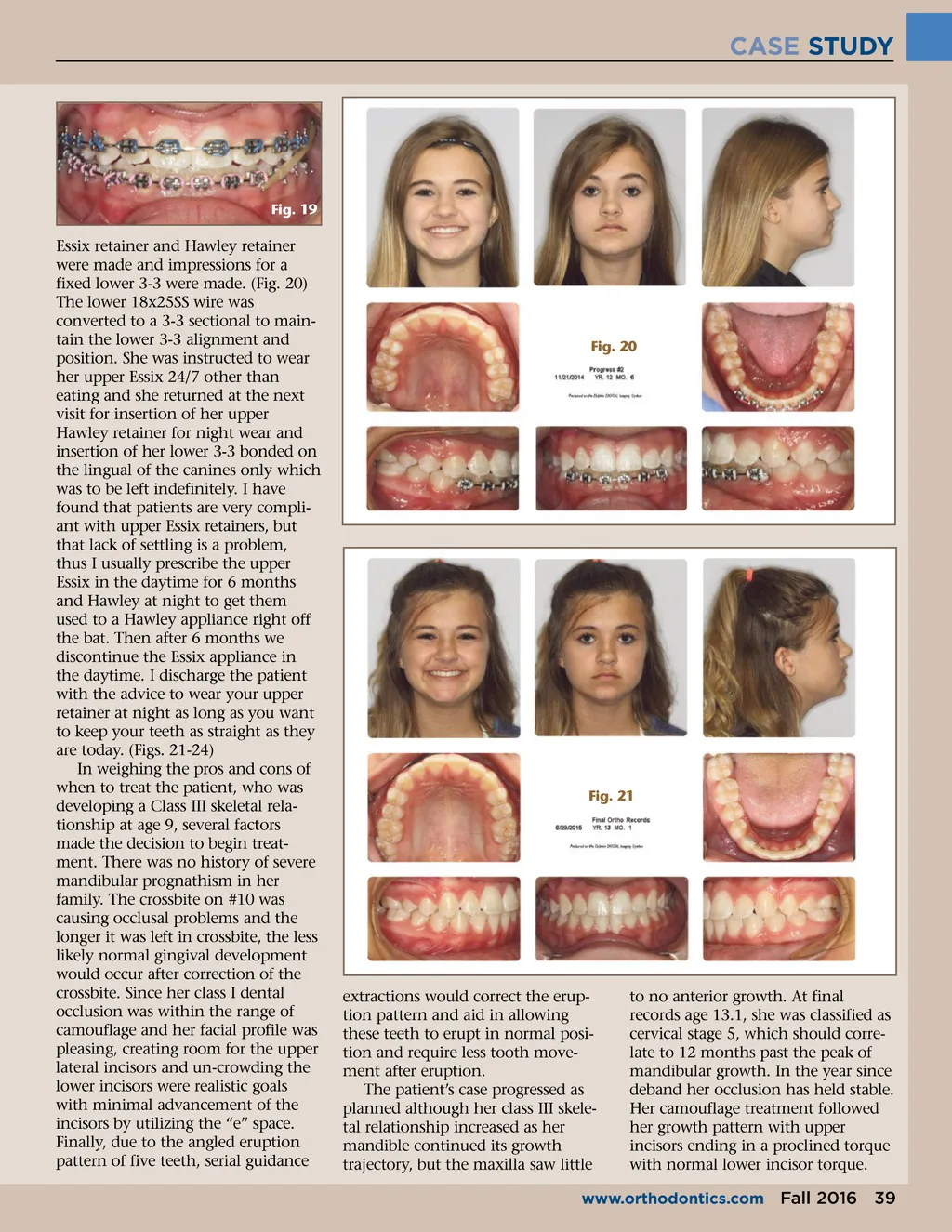
CASE STUDY Fig. 19 Essix retainer and Hawley retainer were made and impressions for a fixed lower 3-3 were made. (Fig. 20) The lower 18x25SS wire was converted to a 3-3 sectional to main-tain the lower 3-3 alignment and position. She was instructed to wear her upper Essix 24/7 other than eating and she returned at the next visit for insertion of her upper Hawley retainer for night wear and insertion of her lower 3-3 bonded on the lingual of the canines only which was to be left indefinitely. I have found that patients are very compli-ant with upper Essix retainers, but that lack of settling is a problem, thus I usually prescribe the upper Essix in the daytime for 6 months and Hawley at night to get them used to a Hawley appliance right off the bat. Then after 6 months we discontinue the Essix appliance in the daytime. I discharge the patient with the advice to wear your upper retainer at night as long as you want to keep your teeth as straight as they are today. (Figs. 21-24) In weighing the pros and cons of when to treat the patient, who was developing a Class III skeletal rela-tionship at age 9, several factors made the decision to begin treat-ment. There was no history of severe mandibular prognathism in her family. The crossbite on #10 was causing occlusal problems and the longer it was left in crossbite, the less likely normal gingival development would occur after correction of the crossbite. Since her class I dental occlusion was within the range of camouflage and her facial profile was pleasing, creating room for the upper lateral incisors and un-crowding the lower incisors were realistic goals with minimal advancement of the incisors by utilizing the “e” space. Finally, due to the angled eruption pattern of five teeth, serial guidance Fig. 20 Fig. 21 extractions would correct the erup-tion pattern and aid in allowing these teeth to erupt in normal posi-tion and require less tooth move-ment after eruption. The patient’s case progressed as planned although her class III skele-tal relationship increased as her mandible continued its growth trajectory, but the maxilla saw little to no anterior growth. At final records age 13.1, she was classified as cervical stage 5, which should corre-late to 12 months past the peak of mandibular growth. In the year since deband her occlusion has held stable. Her camouflage treatment followed her growth pattern with upper incisors ending in a proclined torque with normal lower incisor torque. www.orthodontics.com Fall 2016 39
Journal of the American Orthodontic Society Fall 2016: Page 39