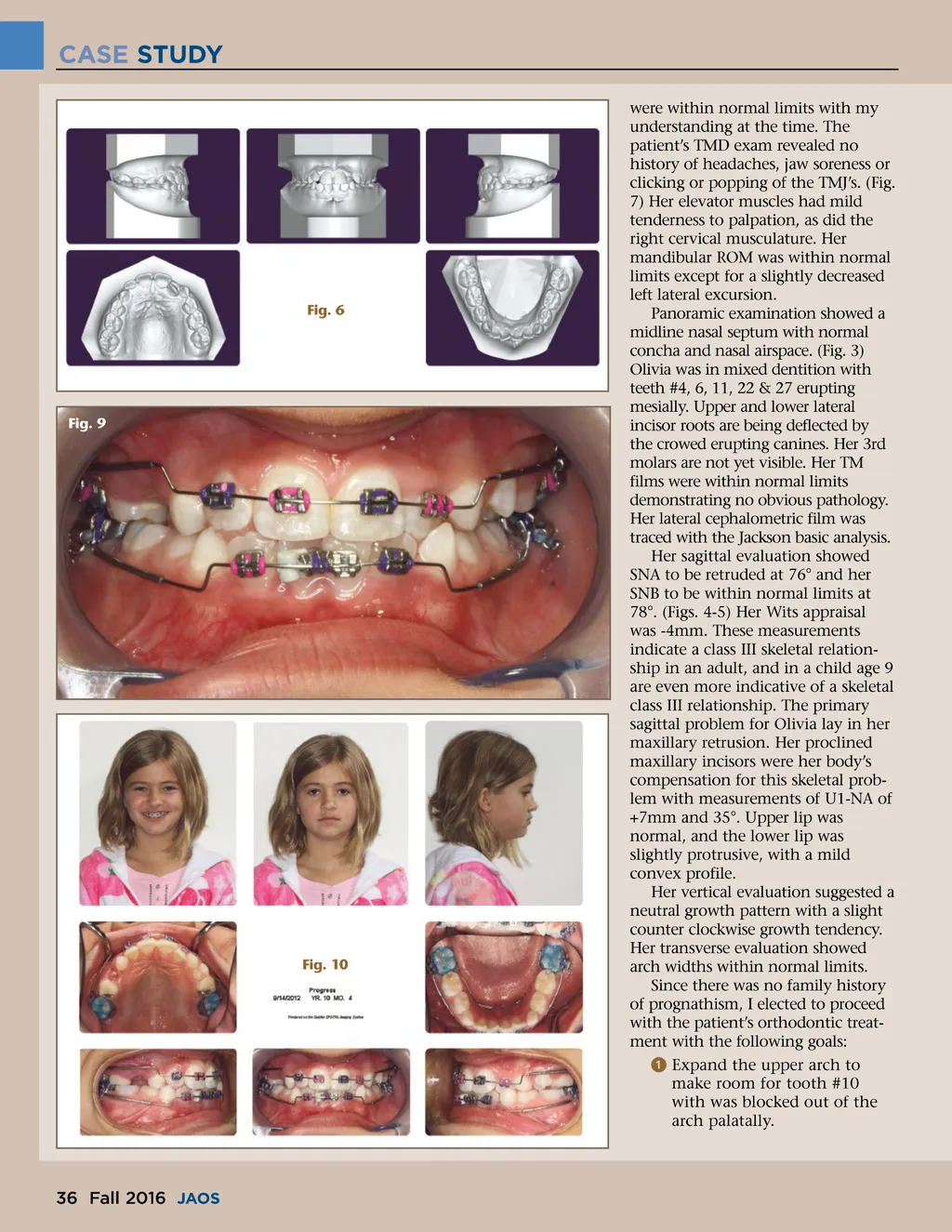
CASE STUDY were within normal limits with my understanding at the time. The patient’s TMD exam revealed no history of headaches, jaw soreness or clicking or popping of the TMJ’s. (Fig. 7) Her elevator muscles had mild tenderness to palpation, as did the right cervical musculature. Her mandibular ROM was within normal limits except for a slightly decreased left lateral excursion. Panoramic examination showed a midline nasal septum with normal concha and nasal airspace. (Fig. 3) Olivia was in mixed dentition with teeth #4, 6, 11, 22 & 27 erupting mesially. Upper and lower lateral incisor roots are being deflected by the crowed erupting canines. Her 3rd molars are not yet visible. Her TM films were within normal limits demonstrating no obvious pathology. Her lateral cephalometric film was traced with the Jackson basic analysis. Her sagittal evaluation showed SNA to be retruded at 76° and her SNB to be within normal limits at 78°. (Figs. 4-5) Her Wits appraisal was -4mm. These measurements indicate a class III skeletal relation-ship in an adult, and in a child age 9 are even more indicative of a skeletal class III relationship. The primary sagittal problem for Olivia lay in her maxillary retrusion. Her proclined maxillary incisors were her body’s compensation for this skeletal prob-lem with measurements of U1-NA of +7mm and 35°. Upper lip was normal, and the lower lip was slightly protrusive, with a mild convex profile. Her vertical evaluation suggested a neutral growth pattern with a slight counter clockwise growth tendency. Her transverse evaluation showed arch widths within normal limits. Since there was no family history of prognathism, I elected to proceed with the patient’s orthodontic treat-ment with the following goals: ᕡ Expand the upper arch to make room for tooth #10 with was blocked out of the arch palatally. Fig. 6 Fig. 9 Fig. 10 36 Fall 2016 JAOS
Journal of the American Orthodontic Society Fall 2016: Page 36