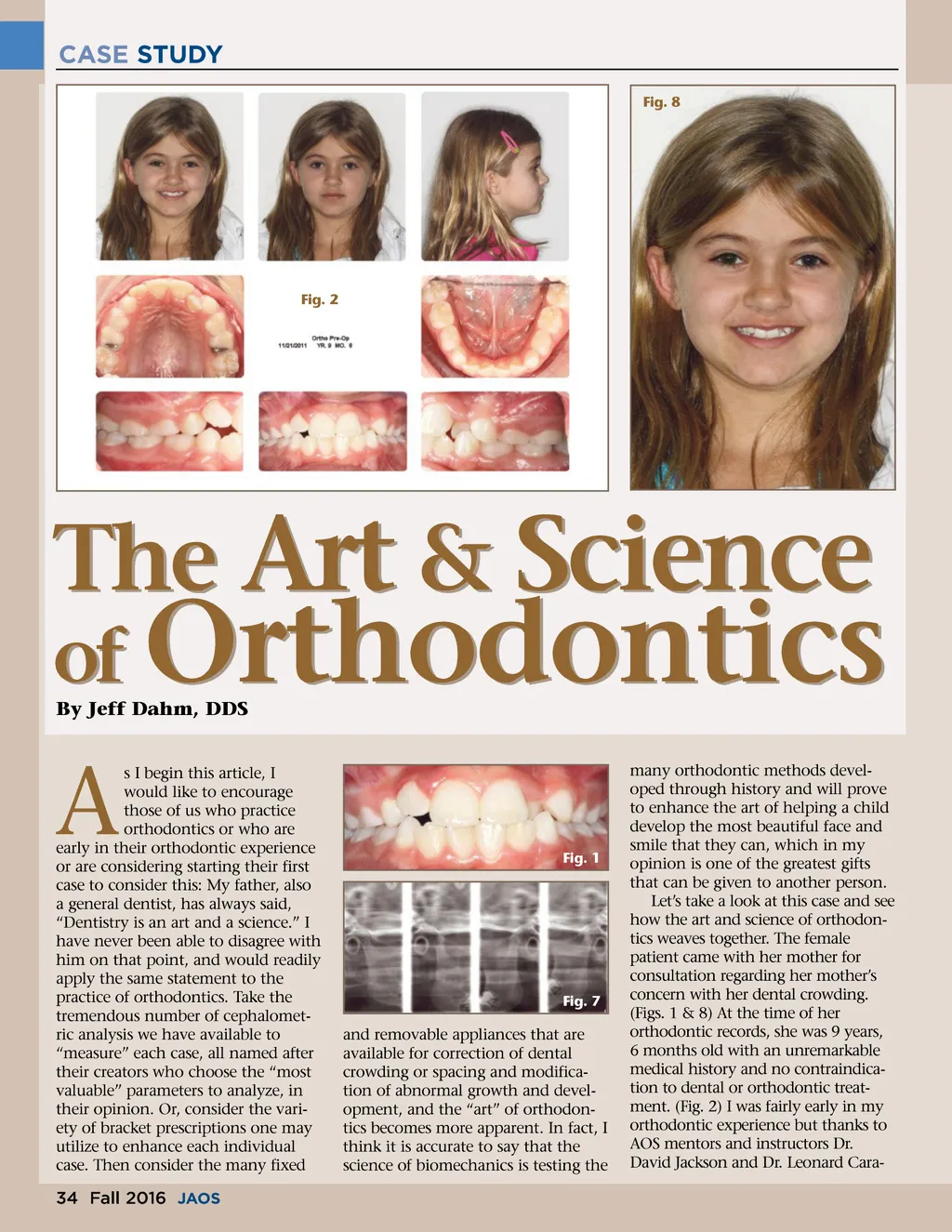
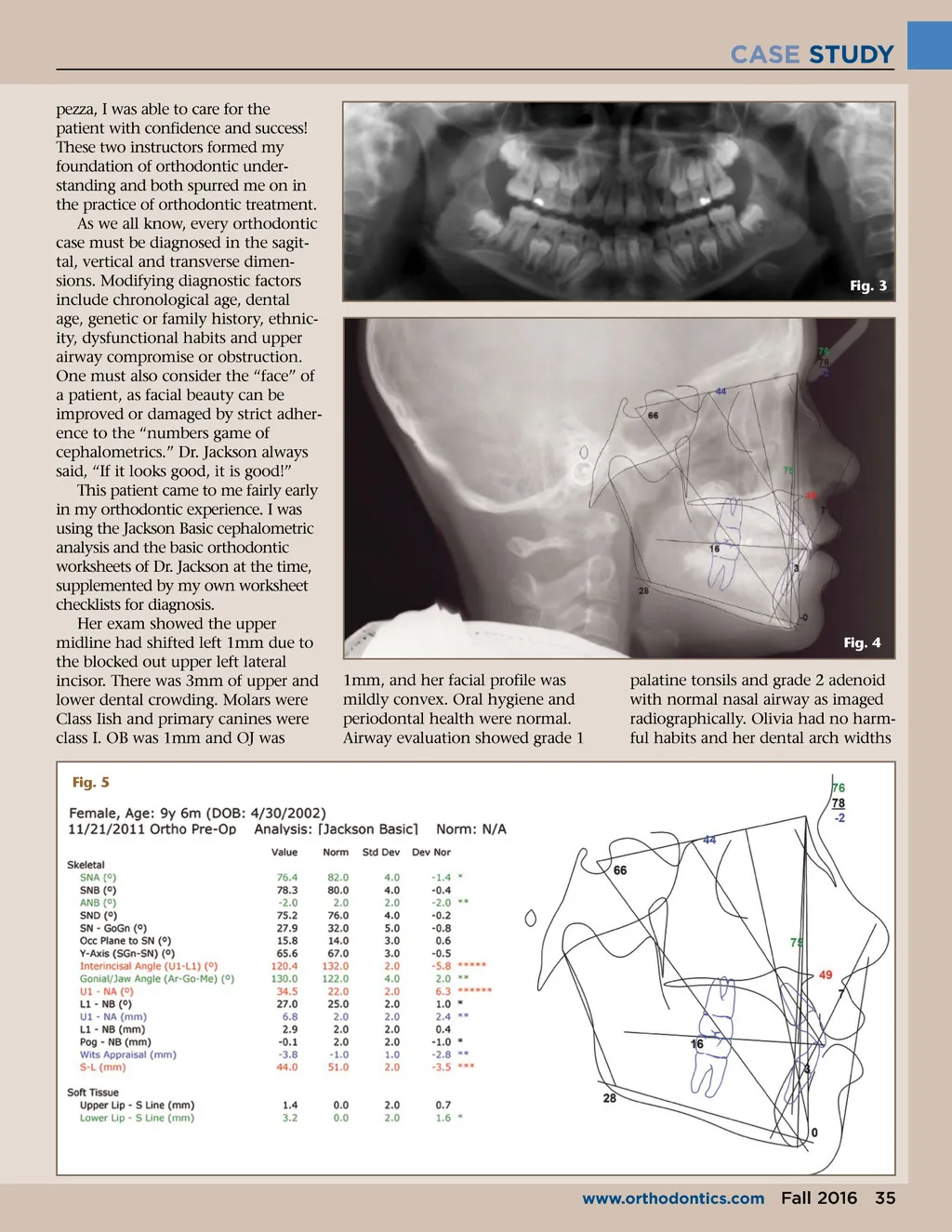
CASE STUDY pezza, I was able to care for the patient with confidence and success! These two instructors formed my foundation of orthodontic under-standing and both spurred me on in the practice of orthodontic treatment. As we all know, every orthodontic case must be diagnosed in the sagit-tal, vertical and transverse dimen-sions. Modifying diagnostic factors include chronological age, dental age, genetic or family history, ethnic-ity, dysfunctional habits and upper airway compromise or obstruction. One must also consider the “face” of a patient, as facial beauty can be improved or damaged by strict adher-ence to the “numbers game of cephalometrics.” Dr. Jackson always said, “If it looks good, it is good!” This patient came to me fairly early in my orthodontic experience. I was using the Jackson Basic cephalometric analysis and the basic orthodontic worksheets of Dr. Jackson at the time, supplemented by my own worksheet checklists for diagnosis. Her exam showed the upper midline had shifted left 1mm due to the blocked out upper left lateral incisor. There was 3mm of upper and lower dental crowding. Molars were Class Iish and primary canines were class I. OB was 1mm and OJ was Fig. 5 Fig. 3 Fig. 4 1mm, and her facial profile was mildly convex. Oral hygiene and periodontal health were normal. Airway evaluation showed grade 1 palatine tonsils and grade 2 adenoid with normal nasal airway as imaged radiographically. Olivia had no harm-ful habits and her dental arch widths www.orthodontics.com Fall 2016 35
Journal of the American Orthodontic Society Fall 2016: Page 35