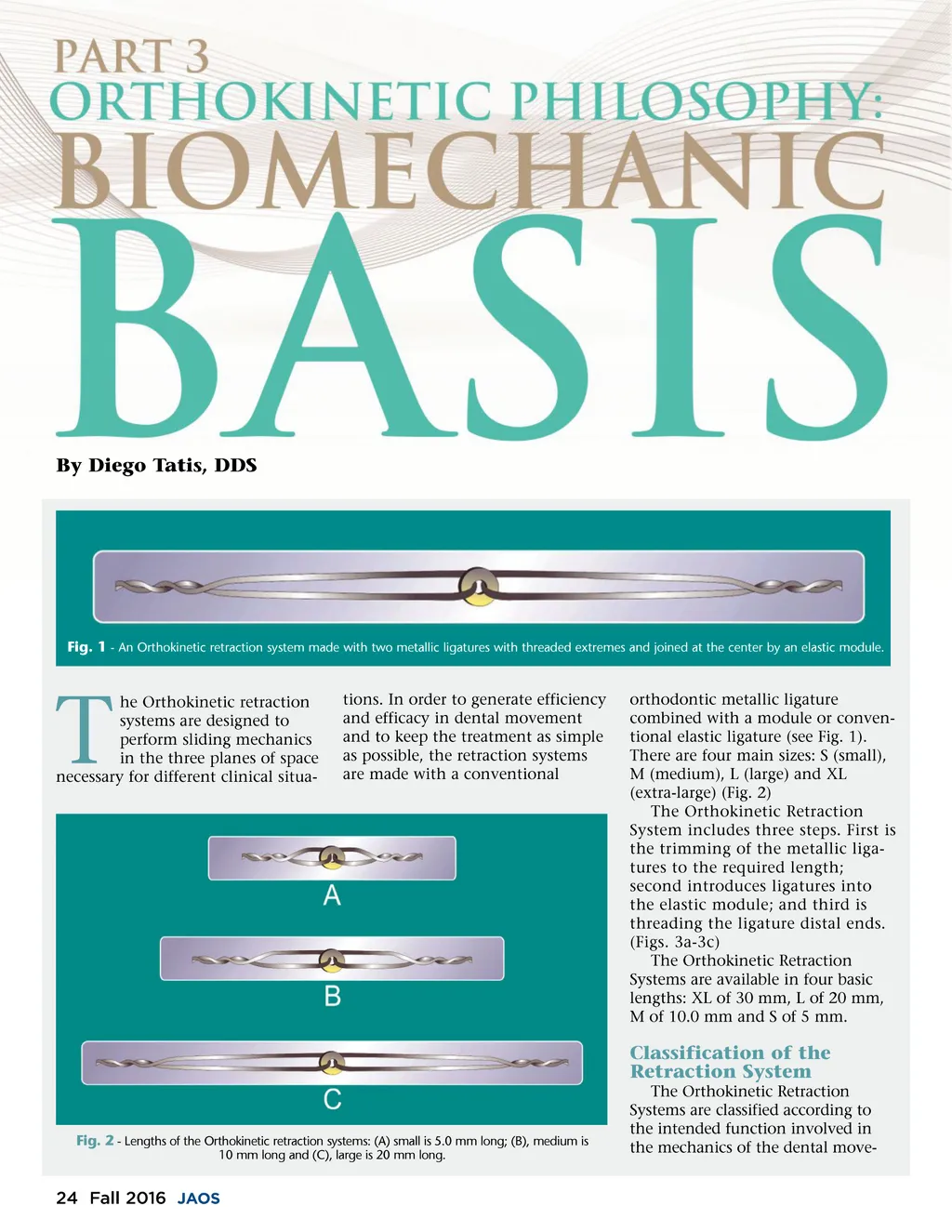
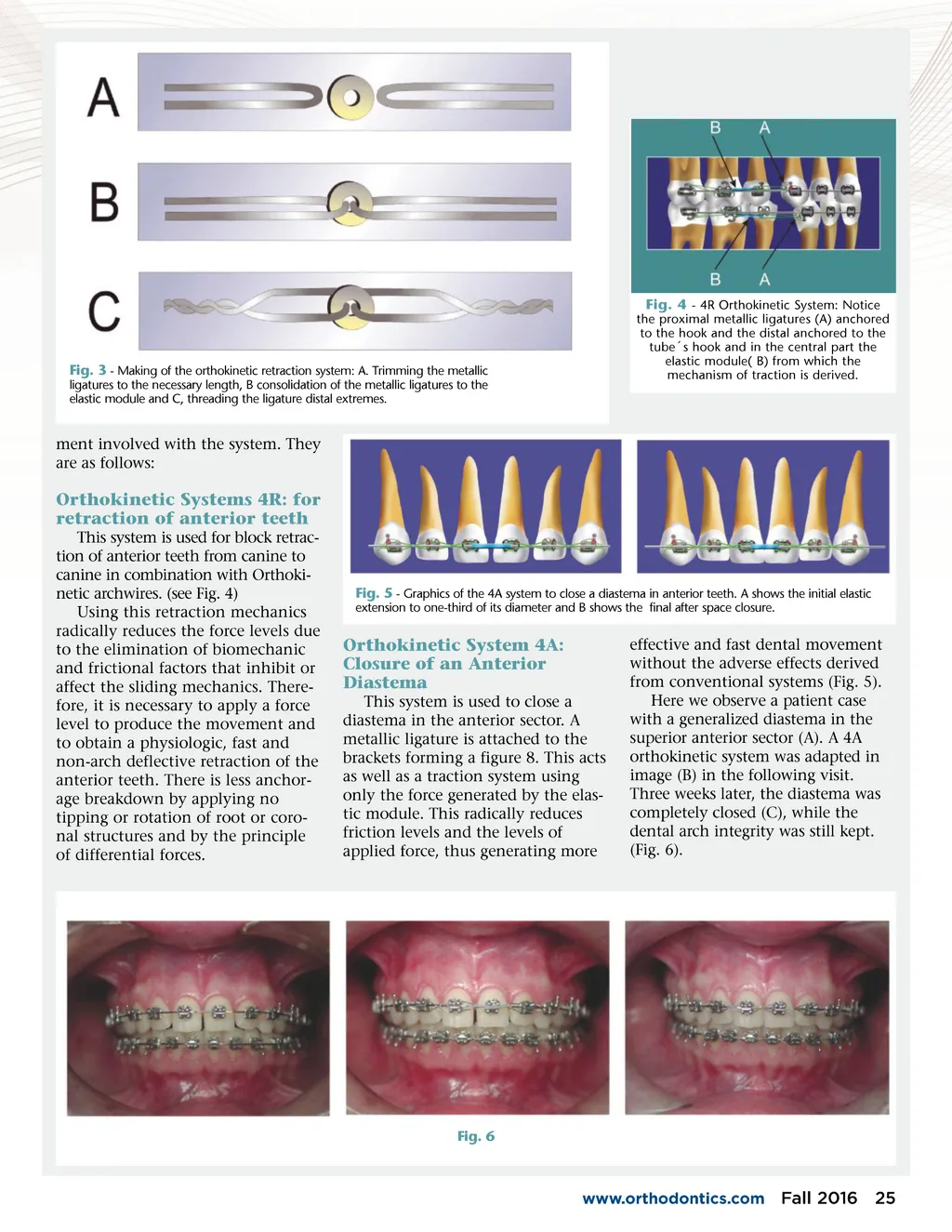
Fig. 3 -Making of the orthokinetic retraction system: A. Trimming the metallic ligatures to the necessary length, B consolidation of the metallic ligatures to the elastic module and C, threading the ligature distal extremes. Fig. 4 -4R Orthokinetic System: Notice the proximal metallic ligatures (A) anchored to the hook and the distal anchored to the tube ´ s hook and in the central part the elastic module( B) from which the mechanism of traction is derived. ment involved with the system. They are as follows: Orthokinetic Systems 4R: for retraction of anterior teeth This system is used for block retrac-tion of anterior teeth from canine to canine in combination with Orthoki-netic archwires. (see Fig. 4) Using this retraction mechanics radically reduces the force levels due to the elimination of biomechanic and frictional factors that inhibit or affect the sliding mechanics. There-fore, it is necessary to apply a force level to produce the movement and to obtain a physiologic, fast and non-arch deflective retraction of the anterior teeth. There is less anchor-age breakdown by applying no tipping or rotation of root or coro-nal structures and by the principle of differential forces. Fig. 5 -Graphics of the 4A system to close a diastema in anterior teeth. A shows the initial elastic extension to one-third of its diameter and B shows the final after space closure. Orthokinetic System 4A: Closure of an Anterior Diastema This system is used to close a diastema in the anterior sector. A metallic ligature is attached to the brackets forming a figure 8. This acts as well as a traction system using only the force generated by the elas-tic module. This radically reduces friction levels and the levels of applied force, thus generating more effective and fast dental movement without the adverse effects derived from conventional systems (Fig. 5). Here we observe a patient case with a generalized diastema in the superior anterior sector (A). A 4A orthokinetic system was adapted in image (B) in the following visit. Three weeks later, the diastema was completely closed (C), while the dental arch integrity was still kept. (Fig. 6). Fig. 6 www.orthodontics.com Fall 2016 25
Journal of the American Orthodontic Society Fall 2016: Page 25