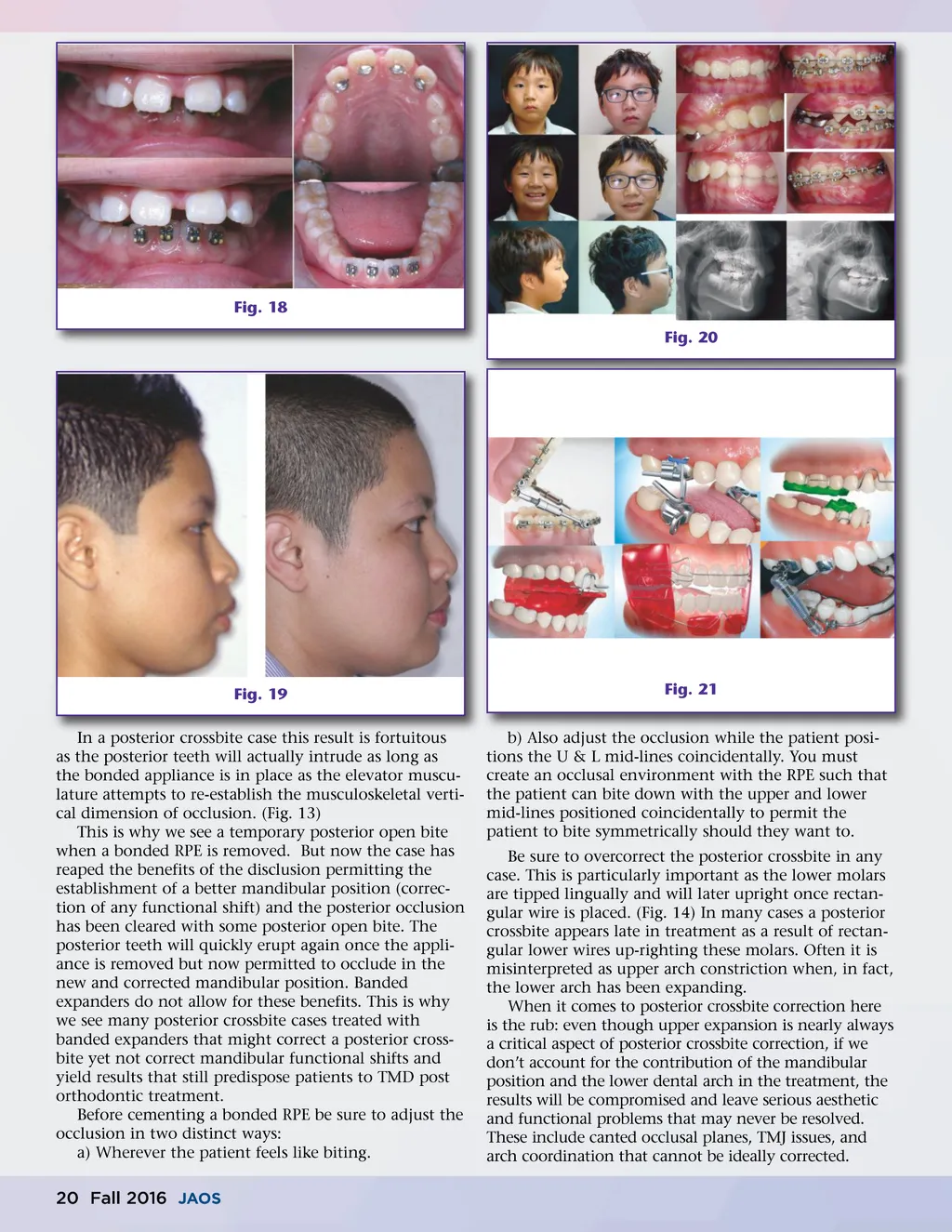
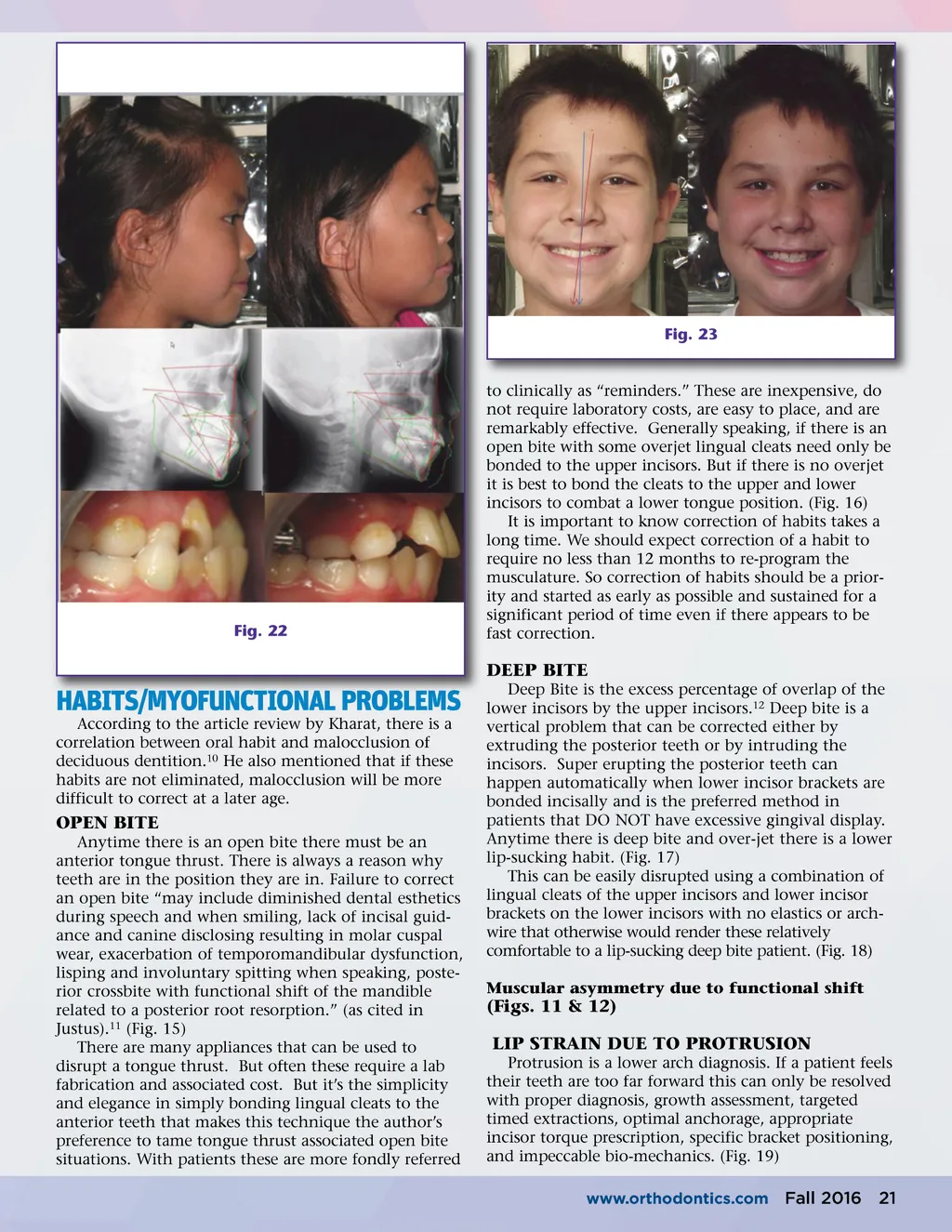
Fig. 23 Fig. 22 to clinically as “reminders.” These are inexpensive, do not require laboratory costs, are easy to place, and are remarkably effective. Generally speaking, if there is an open bite with some overjet lingual cleats need only be bonded to the upper incisors. But if there is no overjet it is best to bond the cleats to the upper and lower incisors to combat a lower tongue position. (Fig. 16) It is important to know correction of habits takes a long time. We should expect correction of a habit to require no less than 12 months to re-program the musculature. So correction of habits should be a prior-ity and started as early as possible and sustained for a significant period of time even if there appears to be fast correction. DEEP BITE HABITS/MYOFUNCTIONAL PROBLEMS According to the article review by Kharat, there is a correlation between oral habit and malocclusion of deciduous dentition. 10 He also mentioned that if these habits are not eliminated, malocclusion will be more difficult to correct at a later age. OPEN BITE Anytime there is an open bite there must be an anterior tongue thrust. There is always a reason why teeth are in the position they are in. Failure to correct an open bite “may include diminished dental esthetics during speech and when smiling, lack of incisal guid-ance and canine disclosing resulting in molar cuspal wear, exacerbation of temporomandibular dysfunction, lisping and involuntary spitting when speaking, poste-rior crossbite with functional shift of the mandible related to a posterior root resorption.” (as cited in Justus). 11 (Fig. 15) There are many appliances that can be used to disrupt a tongue thrust. But often these require a lab fabrication and associated cost. But it’s the simplicity and elegance in simply bonding lingual cleats to the anterior teeth that makes this technique the author’s preference to tame tongue thrust associated open bite situations. With patients these are more fondly referred Deep Bite is the excess percentage of overlap of the lower incisors by the upper incisors. 12 Deep bite is a vertical problem that can be corrected either by extruding the posterior teeth or by intruding the incisors. Super erupting the posterior teeth can happen automatically when lower incisor brackets are bonded incisally and is the preferred method in patients that DO NOT have excessive gingival display. Anytime there is deep bite and over-jet there is a lower lip-sucking habit. (Fig. 17) This can be easily disrupted using a combination of lingual cleats of the upper incisors and lower incisor brackets on the lower incisors with no elastics or arch-wire that otherwise would render these relatively comfortable to a lip-sucking deep bite patient. (Fig. 18) Muscular asymmetry due to functional shift (Figs. 11 & 12) LIP STRAIN DUE TO PROTRUSION Protrusion is a lower arch diagnosis. If a patient feels their teeth are too far forward this can only be resolved with proper diagnosis, growth assessment, targeted timed extractions, optimal anchorage, appropriate incisor torque prescription, specific bracket positioning, and impeccable bio-mechanics. (Fig. 19) www.orthodontics.com Fall 2016 21
Journal of the American Orthodontic Society Fall 2016: Page 21