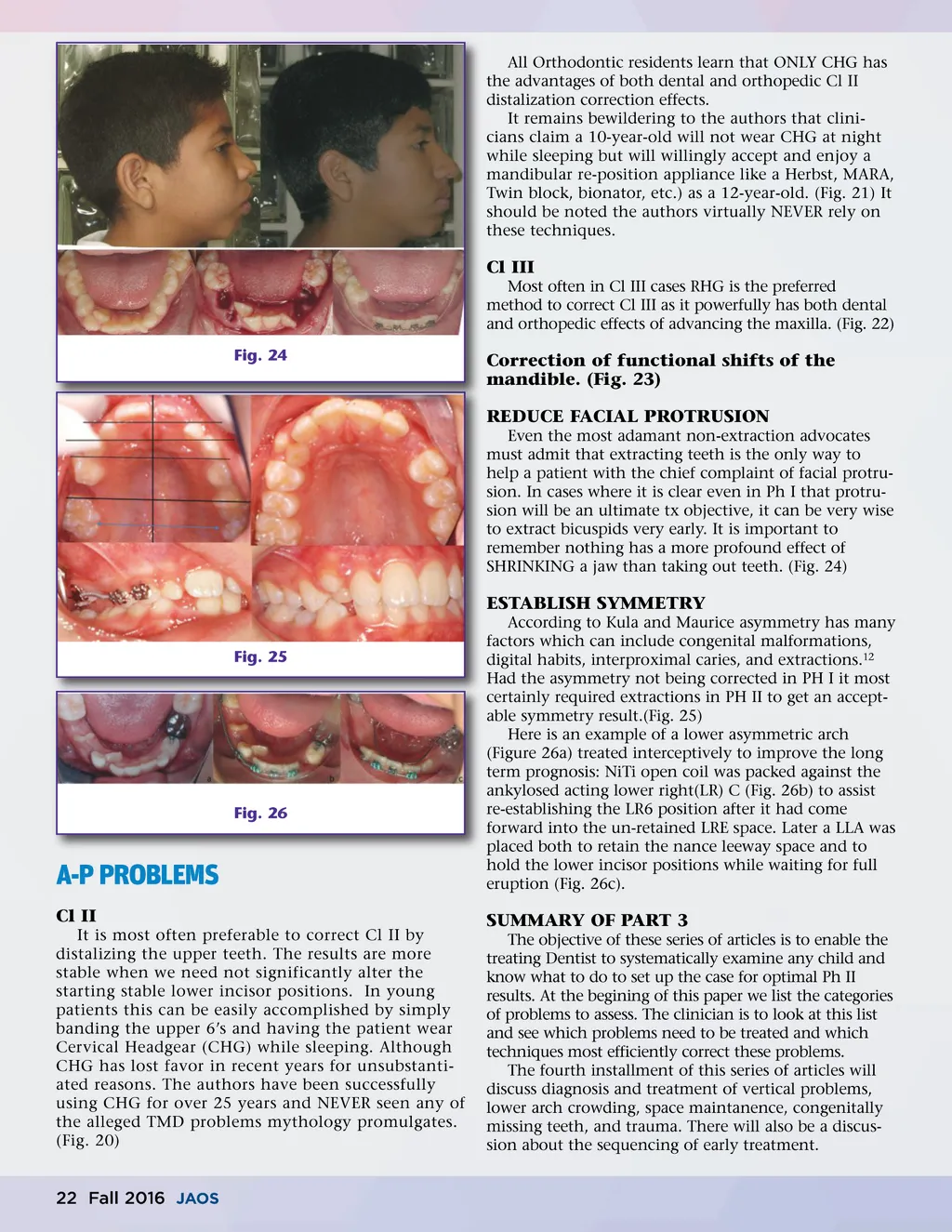
All Orthodontic residents learn that ONLY CHG has the advantages of both dental and orthopedic Cl II distalization correction effects. It remains bewildering to the authors that clini-cians claim a 10-year-old will not wear CHG at night while sleeping but will willingly accept and enjoy a mandibular re-position appliance like a Herbst, MARA, Twin block, bionator, etc.) as a 12-year-old. (Fig. 21) It should be noted the authors virtually NEVER rely on these techniques. Cl III Most often in Cl III cases RHG is the preferred method to correct Cl III as it powerfully has both dental and orthopedic effects of advancing the maxilla. (Fig. 22) Fig. 24 Correction of functional shifts of the mandible. (Fig. 23) REDUCE FACIAL PROTRUSION Even the most adamant non-extraction advocates must admit that extracting teeth is the only way to help a patient with the chief complaint of facial protru-sion. In cases where it is clear even in Ph I that protru-sion will be an ultimate tx objective, it can be very wise to extract bicuspids very early. It is important to remember nothing has a more profound effect of SHRINKING a jaw than taking out teeth. (Fig. 24) ESTABLISH SYMMETRY Fig. 25 According to Kula and Maurice asymmetry has many factors which can include congenital malformations, digital habits, interproximal caries, and extractions. 12 Had the asymmetry not being corrected in PH I it most certainly required extractions in PH II to get an accept-able symmetry result.(Fig. 25) Here is an example of a lower asymmetric arch (Figure 26a) treated interceptively to improve the long term prognosis: NiTi open coil was packed against the ankylosed acting lower right(LR) C (Fig. 26b) to assist re-establishing the LR6 position after it had come forward into the un-retained LRE space. Later a LLA was placed both to retain the nance leeway space and to hold the lower incisor positions while waiting for full eruption (Fig. 26c). Fig. 26 A-P PROBLEMS Cl II It is most often preferable to correct Cl II by distalizing the upper teeth. The results are more stable when we need not significantly alter the starting stable lower incisor positions. In young patients this can be easily accomplished by simply banding the upper 6’s and having the patient wear Cervical Headgear (CHG) while sleeping. Although CHG has lost favor in recent years for unsubstanti-ated reasons. The authors have been successfully using CHG for over 25 years and NEVER seen any of the alleged TMD problems mythology promulgates. (Fig. 20) SUMMARY OF PART 3 The objective of these series of articles is to enable the treating Dentist to systematically examine any child and know what to do to set up the case for optimal Ph II results. At the begining of this paper we list the categories of problems to assess. The clinician is to look at this list and see which problems need to be treated and which techniques most efficiently correct these problems. The fourth installment of this series of articles will discuss diagnosis and treatment of vertical problems, lower arch crowding, space maintanence, congenitally missing teeth, and trauma. There will also be a discus-sion about the sequencing of early treatment. 22 Fall 2016 JAOS
Journal of the American Orthodontic Society Fall 2016: Page 22