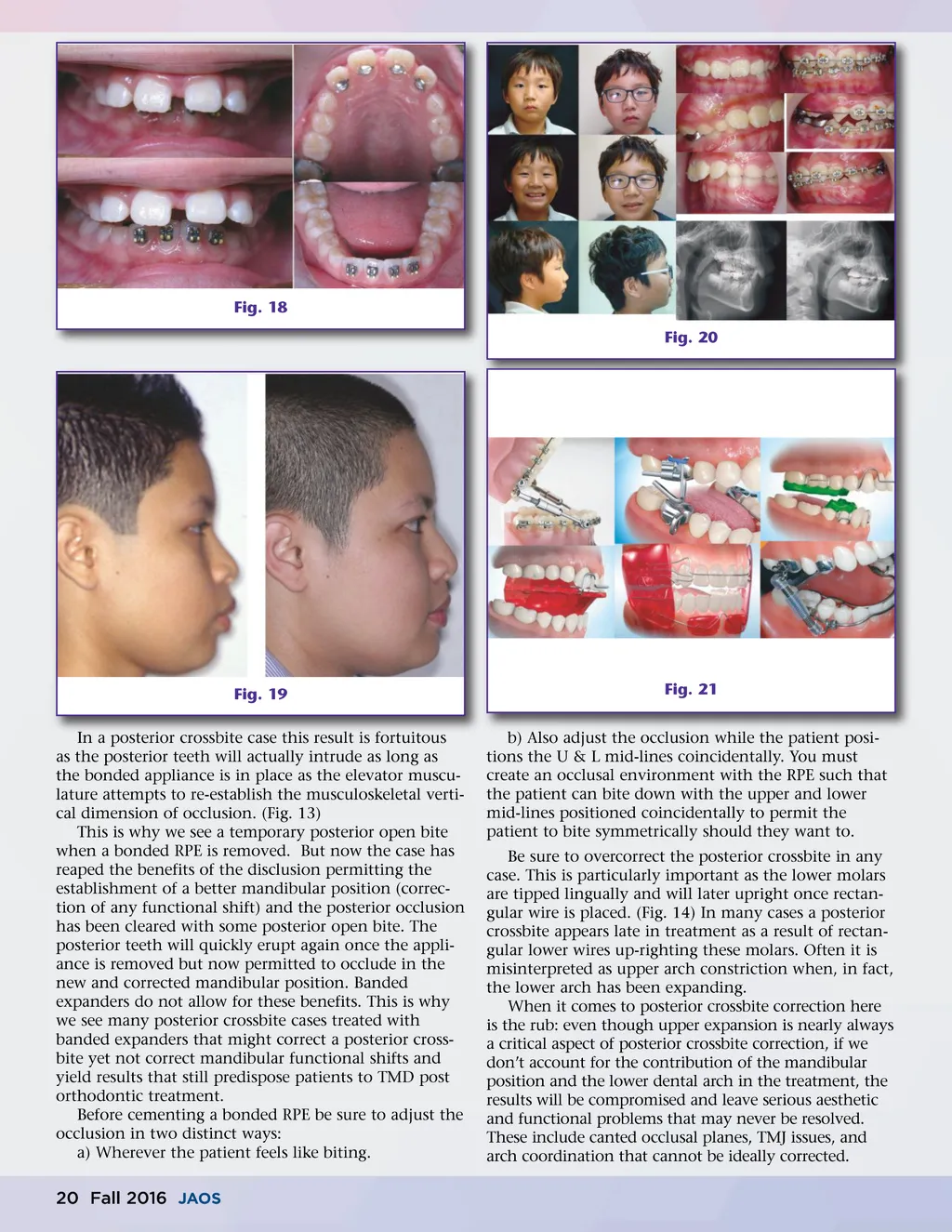
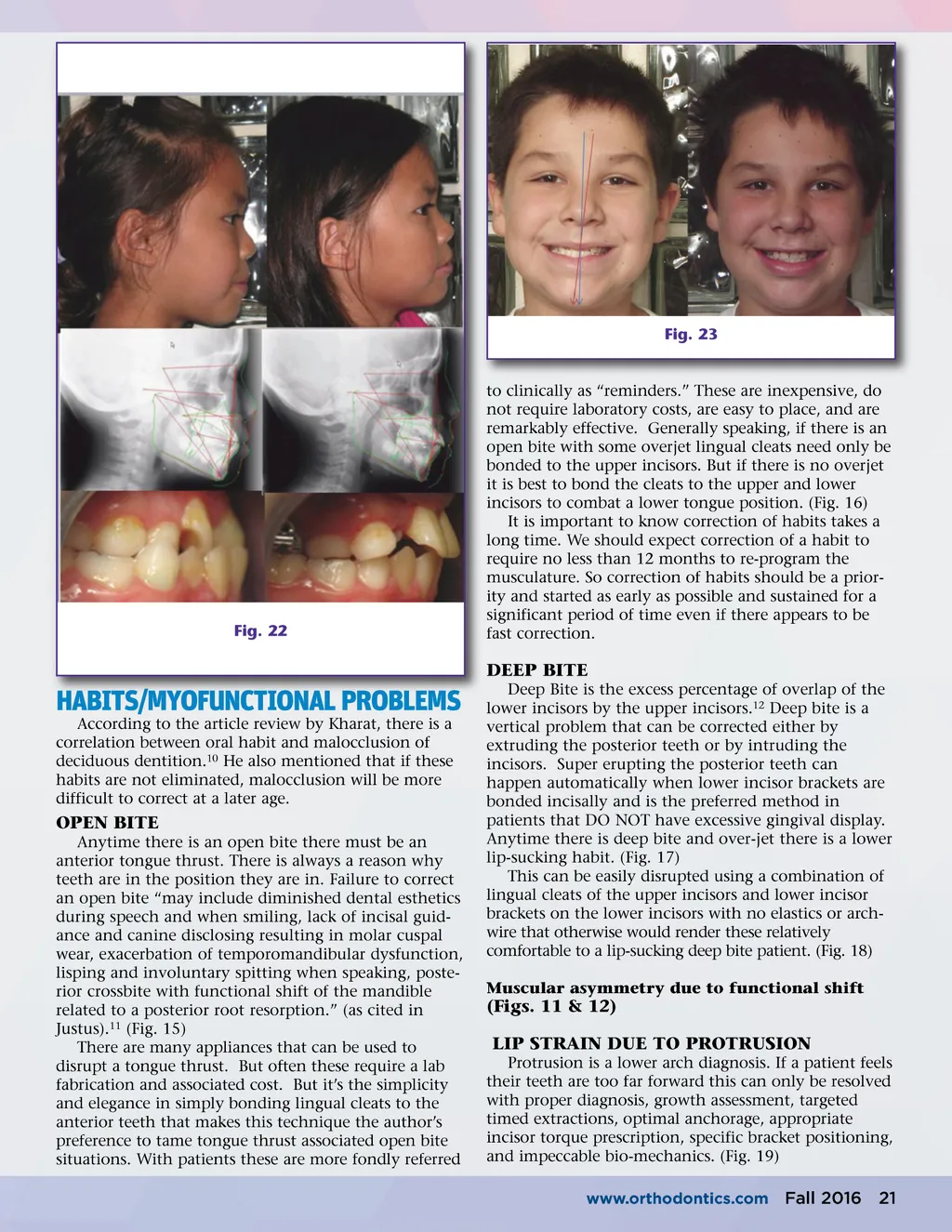
Fig. 18 Fig. 20 Fig. 19 In a posterior crossbite case this result is fortuitous as the posterior teeth will actually intrude as long as the bonded appliance is in place as the elevator muscu-lature attempts to re-establish the musculoskeletal verti-cal dimension of occlusion. (Fig. 13) This is why we see a temporary posterior open bite when a bonded RPE is removed. But now the case has reaped the benefits of the disclusion permitting the establishment of a better mandibular position (correc-tion of any functional shift) and the posterior occlusion has been cleared with some posterior open bite. The posterior teeth will quickly erupt again once the appli-ance is removed but now permitted to occlude in the new and corrected mandibular position. Banded expanders do not allow for these benefits. This is why we see many posterior crossbite cases treated with banded expanders that might correct a posterior cross-bite yet not correct mandibular functional shifts and yield results that still predispose patients to TMD post orthodontic treatment. Before cementing a bonded RPE be sure to adjust the occlusion in two distinct ways: a) Wherever the patient feels like biting. Fig. 21 b) Also adjust the occlusion while the patient posi-tions the U & L mid-lines coincidentally. You must create an occlusal environment with the RPE such that the patient can bite down with the upper and lower mid-lines positioned coincidentally to permit the patient to bite symmetrically should they want to. Be sure to overcorrect the posterior crossbite in any case. This is particularly important as the lower molars are tipped lingually and will later upright once rectan-gular wire is placed. (Fig. 14) In many cases a posterior crossbite appears late in treatment as a result of rectan-gular lower wires up-righting these molars. Often it is misinterpreted as upper arch constriction when, in fact, the lower arch has been expanding. When it comes to posterior crossbite correction here is the rub: even though upper expansion is nearly always a critical aspect of posterior crossbite correction, if we don’t account for the contribution of the mandibular position and the lower dental arch in the treatment, the results will be compromised and leave serious aesthetic and functional problems that may never be resolved. These include canted occlusal planes, TMJ issues, and arch coordination that cannot be ideally corrected. 20 Fall 2016 JAOS
Journal of the American Orthodontic Society Fall 2016: Page 20