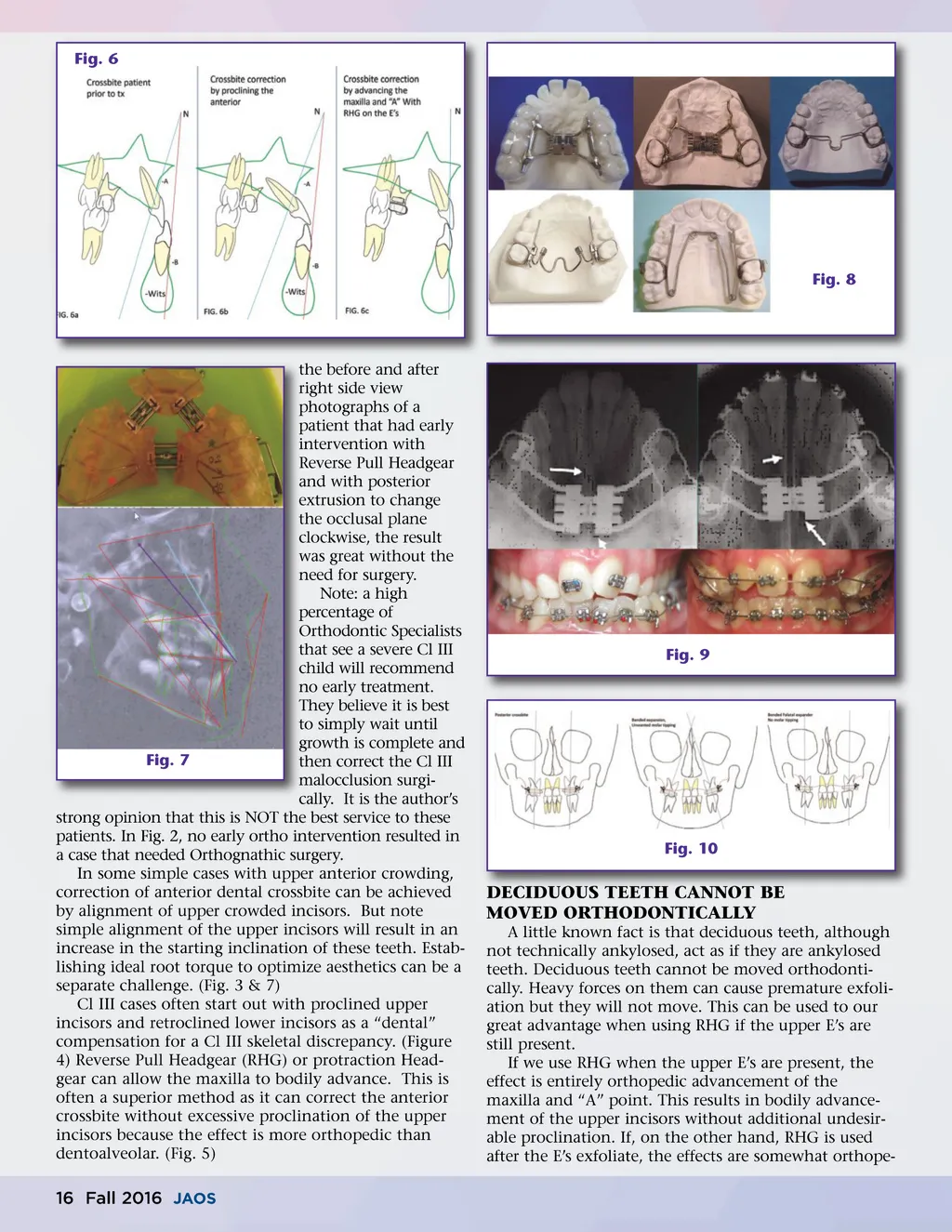
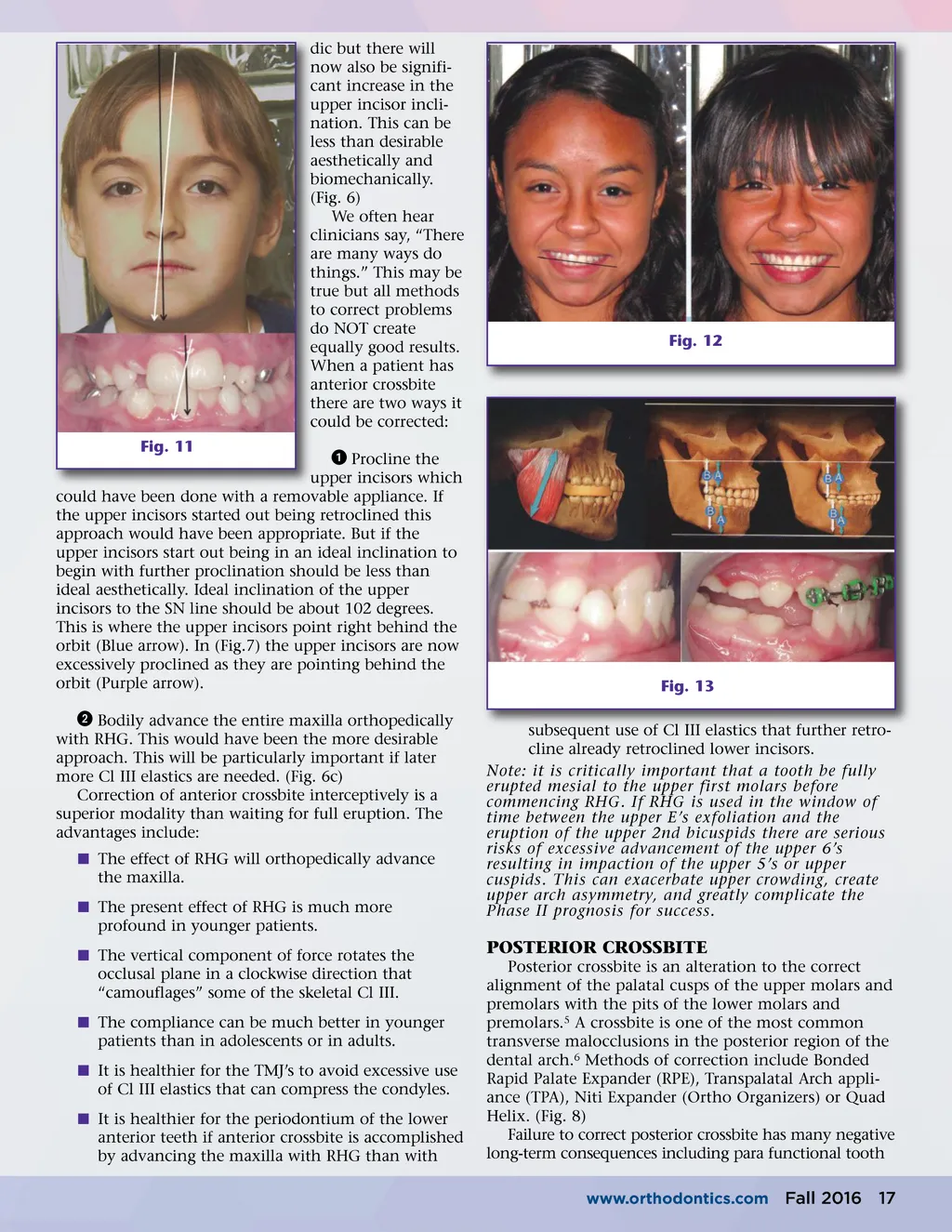
dic but there will now also be signifi-cant increase in the upper incisor incli-nation. This can be less than desirable aesthetically and biomechanically. (Fig. 6) We often hear clinicians say, “There are many ways do things.” This may be true but all methods to correct problems do NOT create equally good results. When a patient has anterior crossbite there are two ways it could be corrected: ᕡ Procline the upper incisors which could have been done with a removable appliance. If the upper incisors started out being retroclined this approach would have been appropriate. But if the upper incisors start out being in an ideal inclination to begin with further proclination should be less than ideal aesthetically. Ideal inclination of the upper incisors to the SN line should be about 102 degrees. This is where the upper incisors point right behind the orbit (Blue arrow). In (Fig.7) the upper incisors are now excessively proclined as they are pointing behind the orbit (Purple arrow). ᕢ Bodily advance the entire maxilla orthopedically with RHG. This would have been the more desirable approach. This will be particularly important if later more Cl III elastics are needed. (Fig. 6c) Correction of anterior crossbite interceptively is a superior modality than waiting for full eruption. The advantages include: í The effect of RHG will orthopedically advance the maxilla. í The present effect of RHG is much more profound in younger patients. í The vertical component of force rotates the occlusal plane in a clockwise direction that “camouflages” some of the skeletal Cl III. í The compliance can be much better in younger patients than in adolescents or in adults. í It is healthier for the TMJ’s to avoid excessive use of Cl III elastics that can compress the condyles. í It is healthier for the periodontium of the lower anterior teeth if anterior crossbite is accomplished by advancing the maxilla with RHG than with Fig. 11 Fig. 12 Fig. 13 subsequent use of Cl III elastics that further retro-cline already retroclined lower incisors. Note: it is critically important that a tooth be fully erupted mesial to the upper first molars before commencing RHG. If RHG is used in the window of time between the upper E’s exfoliation and the eruption of the upper 2nd bicuspids there are serious risks of excessive advancement of the upper 6’s resulting in impaction of the upper 5’s or upper cuspids. This can exacerbate upper crowding, create upper arch asymmetry, and greatly complicate the Phase II prognosis for success. POSTERIOR CROSSBITE Posterior crossbite is an alteration to the correct alignment of the palatal cusps of the upper molars and premolars with the pits of the lower molars and premolars. 5 A crossbite is one of the most common transverse malocclusions in the posterior region of the dental arch. 6 Methods of correction include Bonded Rapid Palate Expander (RPE), Transpalatal Arch appli-ance (TPA), Niti Expander (Ortho Organizers) or Quad Helix. (Fig. 8) Failure to correct posterior crossbite has many negative long-term consequences including para functional tooth www.orthodontics.com Fall 2016 17
Journal of the American Orthodontic Society Fall 2016: Page 17