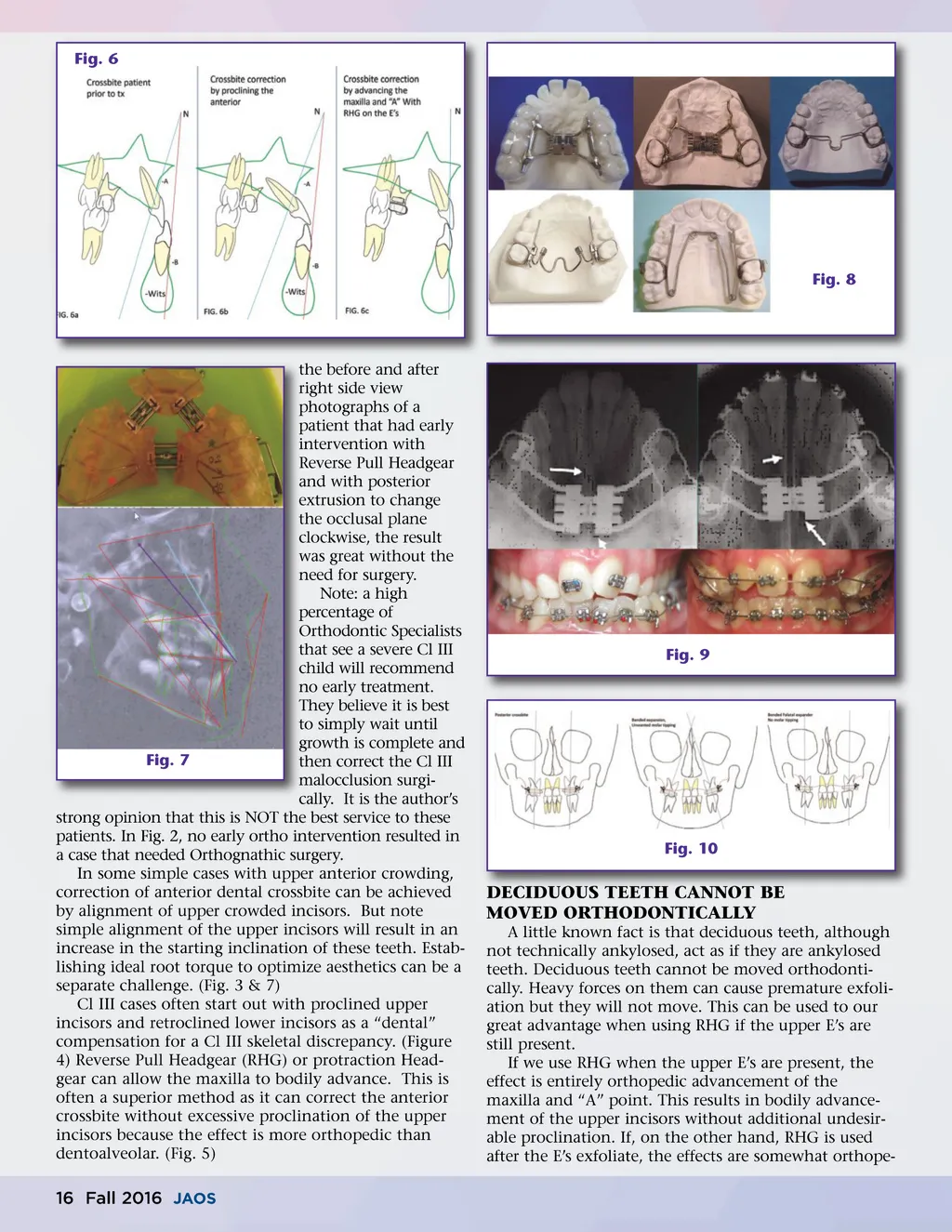
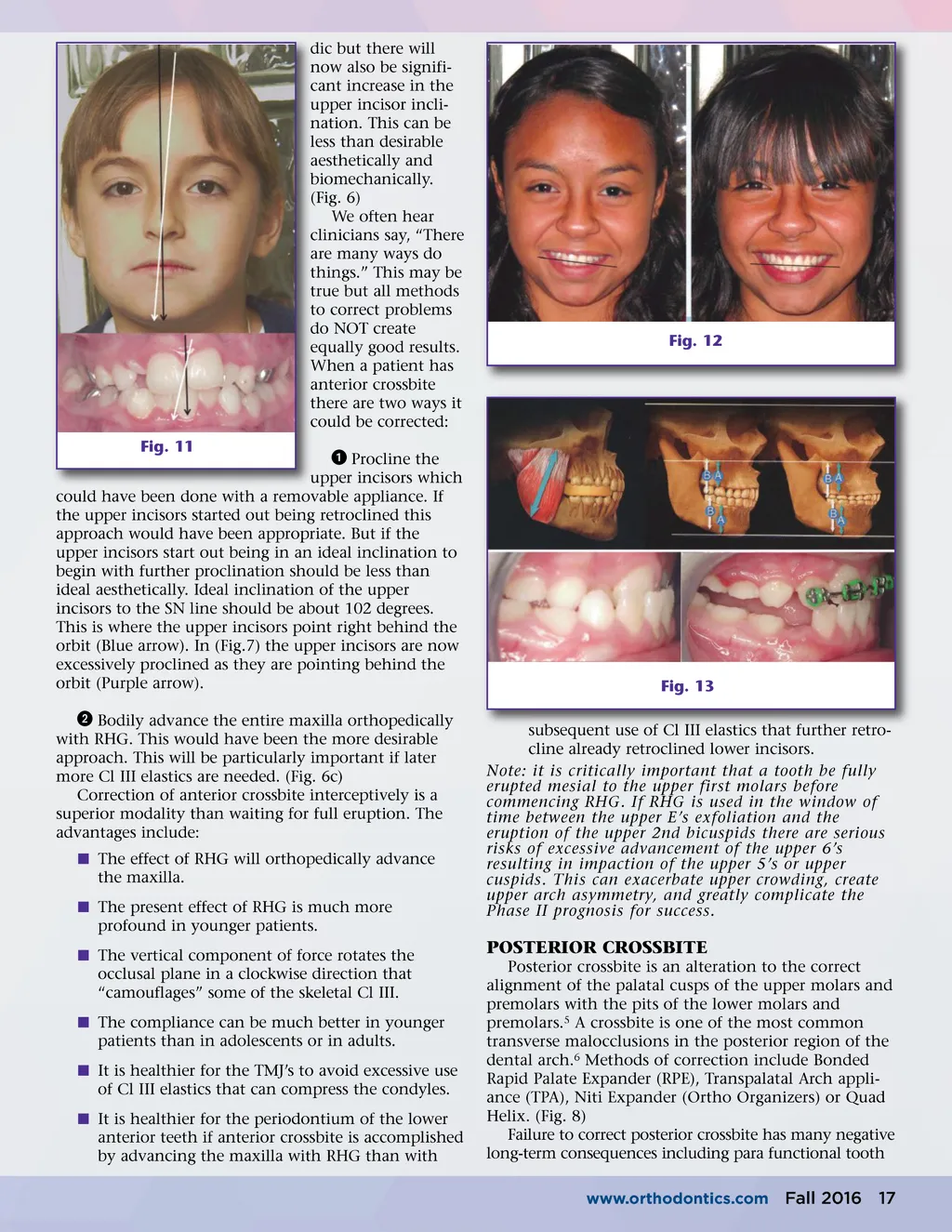
Fig. 6 Fig. 8 the before and after right side view photographs of a patient that had early intervention with Reverse Pull Headgear and with posterior extrusion to change the occlusal plane clockwise, the result was great without the need for surgery. Note: a high percentage of Orthodontic Specialists that see a severe Cl III child will recommend no early treatment. They believe it is best to simply wait until growth is complete and Fig. 7 then correct the Cl III malocclusion surgi-cally. It is the author’s strong opinion that this is NOT the best service to these patients. In Fig. 2, no early ortho intervention resulted in a case that needed Orthognathic surgery. In some simple cases with upper anterior crowding, correction of anterior dental crossbite can be achieved by alignment of upper crowded incisors. But note simple alignment of the upper incisors will result in an increase in the starting inclination of these teeth. Estab-lishing ideal root torque to optimize aesthetics can be a separate challenge. (Fig. 3 & 7) Cl III cases often start out with proclined upper incisors and retroclined lower incisors as a “dental” compensation for a Cl III skeletal discrepancy. (Figure 4) Reverse Pull Headgear (RHG) or protraction Head-gear can allow the maxilla to bodily advance. This is often a superior method as it can correct the anterior crossbite without excessive proclination of the upper incisors because the effect is more orthopedic than dentoalveolar. (Fig. 5) Fig. 9 Fig. 10 DECIDUOUS TEETH CANNOT BE MOVED ORTHODONTICALLY A little known fact is that deciduous teeth, although not technically ankylosed, act as if they are ankylosed teeth. Deciduous teeth cannot be moved orthodonti-cally. Heavy forces on them can cause premature exfoli-ation but they will not move. This can be used to our great advantage when using RHG if the upper E’s are still present. If we use RHG when the upper E’s are present, the effect is entirely orthopedic advancement of the maxilla and “A” point. This results in bodily advance-ment of the upper incisors without additional undesir-able proclination. If, on the other hand, RHG is used after the E’s exfoliate, the effects are somewhat orthope-16 Fall 2016 JAOS
Journal of the American Orthodontic Society Fall 2016: Page 16