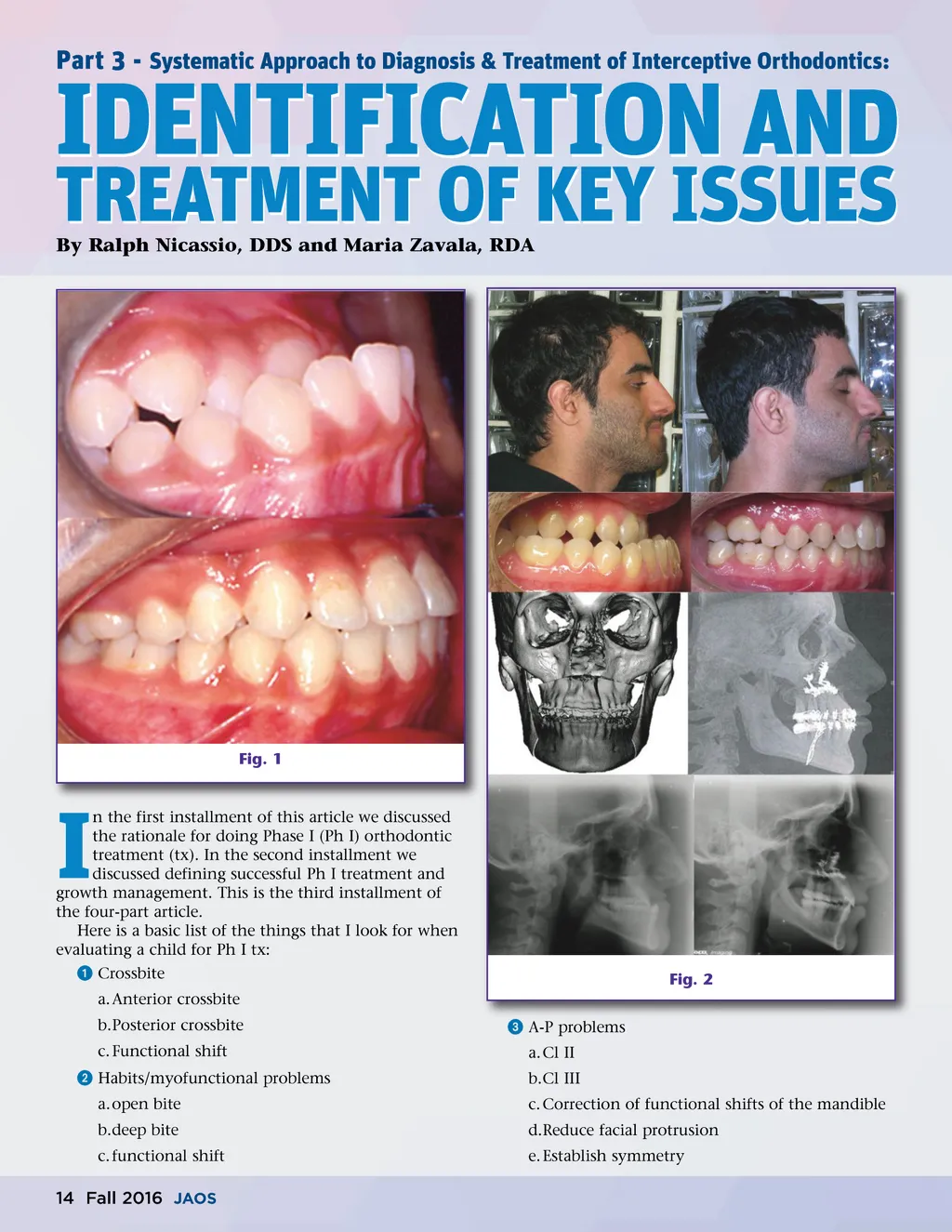
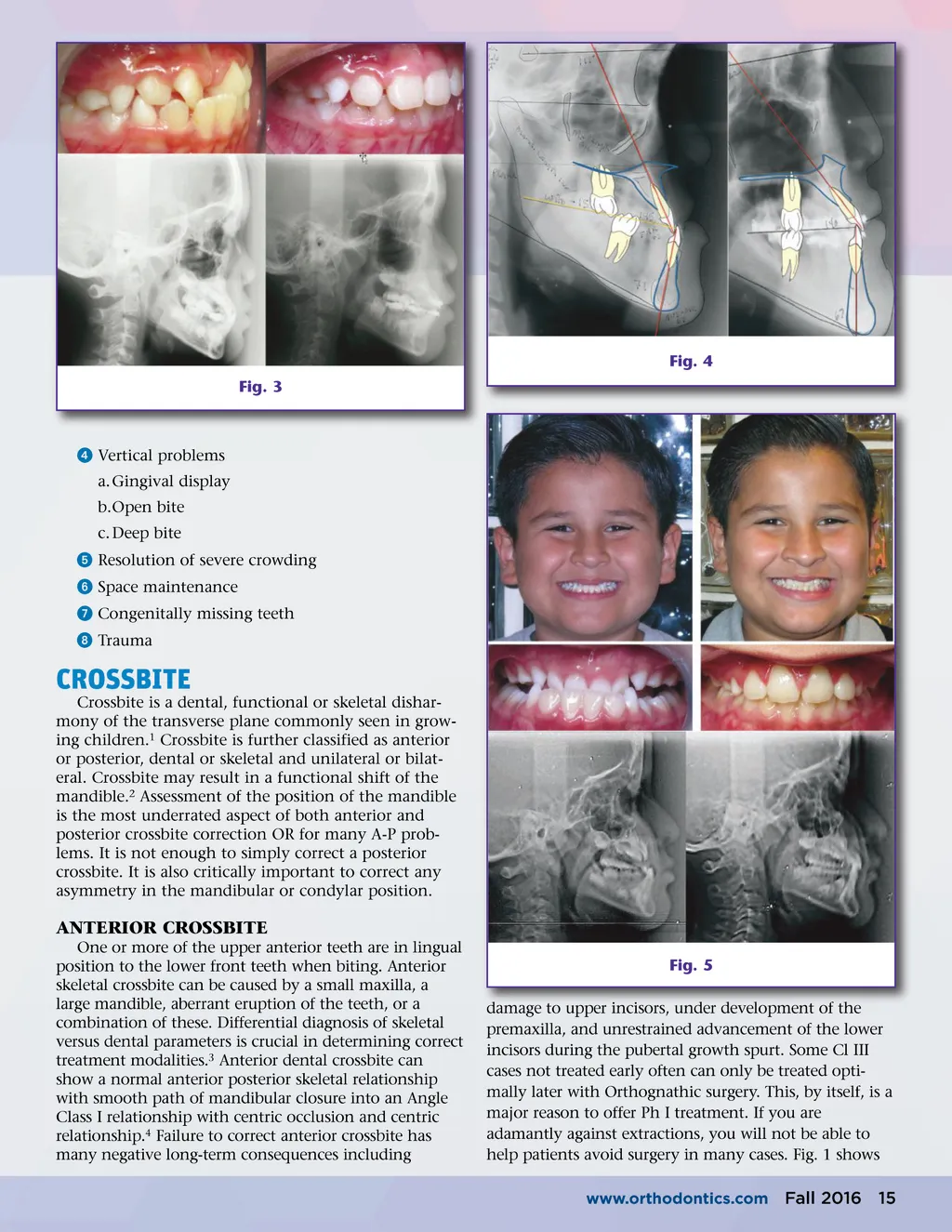
Fig. 4 Fig. 3 ᕤ Vertical problems a. Gingival display b.Open bite c. Deep bite ᕥ Resolution of severe crowding ᕦ Space maintenance ᕧ Congenitally missing teeth ᕨ Trauma CROSSBITE Crossbite is a dental, functional or skeletal dishar-mony of the transverse plane commonly seen in grow-ing children. 1 Crossbite is further classified as anterior or posterior, dental or skeletal and unilateral or bilat-eral. Crossbite may result in a functional shift of the mandible. 2 Assessment of the position of the mandible is the most underrated aspect of both anterior and posterior crossbite correction OR for many A-P prob-lems. It is not enough to simply correct a posterior crossbite. It is also critically important to correct any asymmetry in the mandibular or condylar position. ANTERIOR CROSSBITE One or more of the upper anterior teeth are in lingual position to the lower front teeth when biting. Anterior skeletal crossbite can be caused by a small maxilla, a large mandible, aberrant eruption of the teeth, or a combination of these. Differential diagnosis of skeletal versus dental parameters is crucial in determining correct treatment modalities. 3 Anterior dental crossbite can show a normal anterior posterior skeletal relationship with smooth path of mandibular closure into an Angle Class I relationship with centric occlusion and centric relationship. 4 Failure to correct anterior crossbite has many negative long-term consequences including Fig. 5 damage to upper incisors, under development of the premaxilla, and unrestrained advancement of the lower incisors during the pubertal growth spurt. Some Cl III cases not treated early often can only be treated opti-mally later with Orthognathic surgery. This, by itself, is a major reason to offer Ph I treatment. If you are adamantly against extractions, you will not be able to help patients avoid surgery in many cases. Fig. 1 shows www.orthodontics.com Fall 2016 15
Journal of the American Orthodontic Society Fall 2016: Page 15