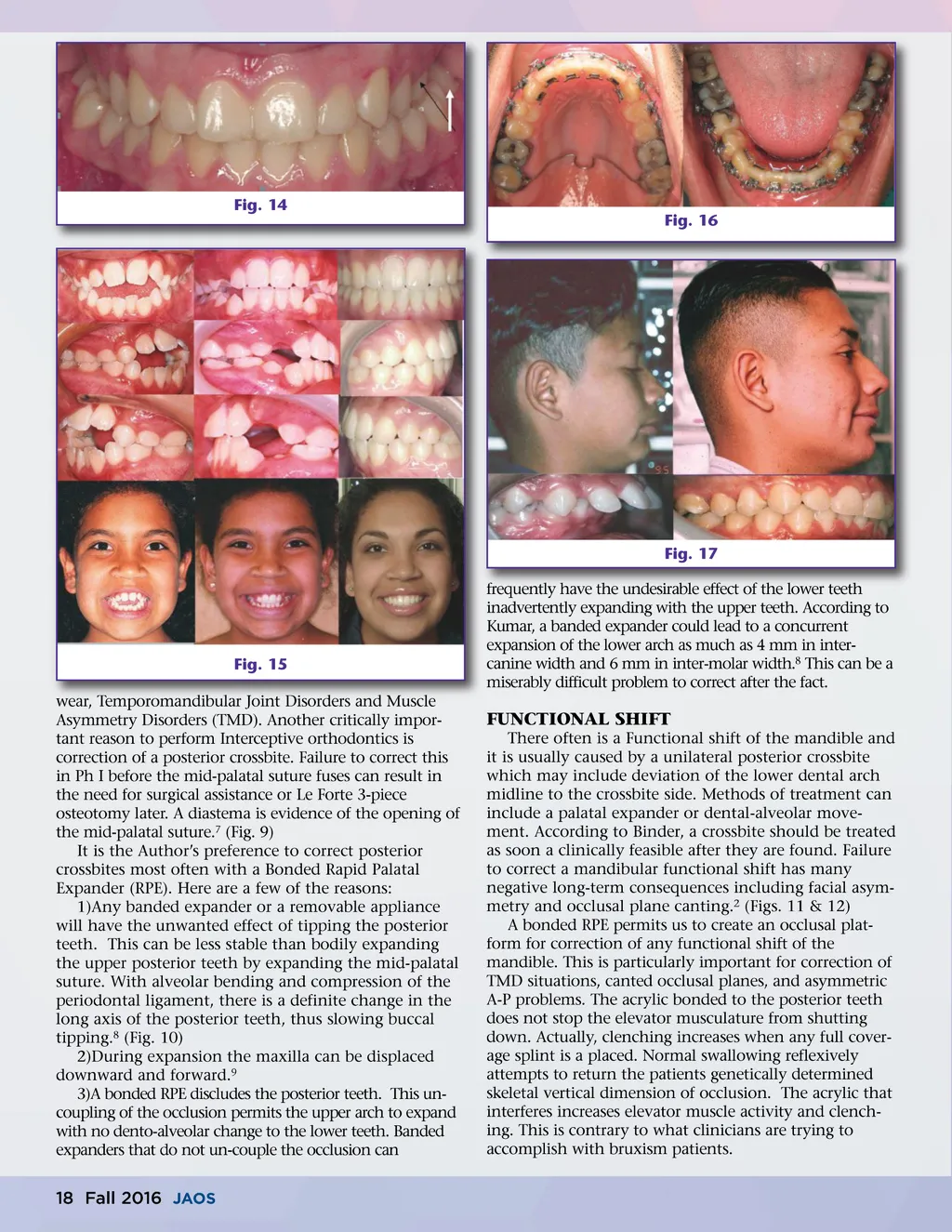
Fig. 14 Fig. 16 Fig. 17 frequently have the undesirable effect of the lower teeth inadvertently expanding with the upper teeth. According to Kumar, a banded expander could lead to a concurrent expansion of the lower arch as much as 4 mm in inter-canine width and 6 mm in inter-molar width. 8 This can be a miserably difficult problem to correct after the fact. Fig. 15 wear, Temporomandibular Joint Disorders and Muscle Asymmetry Disorders (TMD). Another critically impor-tant reason to perform Interceptive orthodontics is correction of a posterior crossbite. Failure to correct this in Ph I before the mid-palatal suture fuses can result in the need for surgical assistance or Le Forte 3-piece osteotomy later. A diastema is evidence of the opening of the mid-palatal suture. 7 (Fig. 9) It is the Author’s preference to correct posterior crossbites most often with a Bonded Rapid Palatal Expander (RPE). Here are a few of the reasons: 1)Any banded expander or a removable appliance will have the unwanted effect of tipping the posterior teeth. This can be less stable than bodily expanding the upper posterior teeth by expanding the mid-palatal suture. With alveolar bending and compression of the periodontal ligament, there is a definite change in the long axis of the posterior teeth, thus slowing buccal tipping. 8 (Fig. 10) 2)During expansion the maxilla can be displaced downward and forward. 9 3)A bonded RPE discludes the posterior teeth. This un-coupling of the occlusion permits the upper arch to expand with no dento-alveolar change to the lower teeth. Banded expanders that do not un-couple the occlusion can FUNCTIONAL SHIFT There often is a Functional shift of the mandible and it is usually caused by a unilateral posterior crossbite which may include deviation of the lower dental arch midline to the crossbite side. Methods of treatment can include a palatal expander or dental-alveolar move-ment. According to Binder, a crossbite should be treated as soon a clinically feasible after they are found. Failure to correct a mandibular functional shift has many negative long-term consequences including facial asym-metry and occlusal plane canting. 2 (Figs. 11 & 12) A bonded RPE permits us to create an occlusal plat-form for correction of any functional shift of the mandible. This is particularly important for correction of TMD situations, canted occlusal planes, and asymmetric A-P problems. The acrylic bonded to the posterior teeth does not stop the elevator musculature from shutting down. Actually, clenching increases when any full cover-age splint is a placed. Normal swallowing reflexively attempts to return the patients genetically determined skeletal vertical dimension of occlusion. The acrylic that interferes increases elevator muscle activity and clench-ing. This is contrary to what clinicians are trying to accomplish with bruxism patients. 18 Fall 2016 JAOS
Journal of the American Orthodontic Society Fall 2016: Page 18