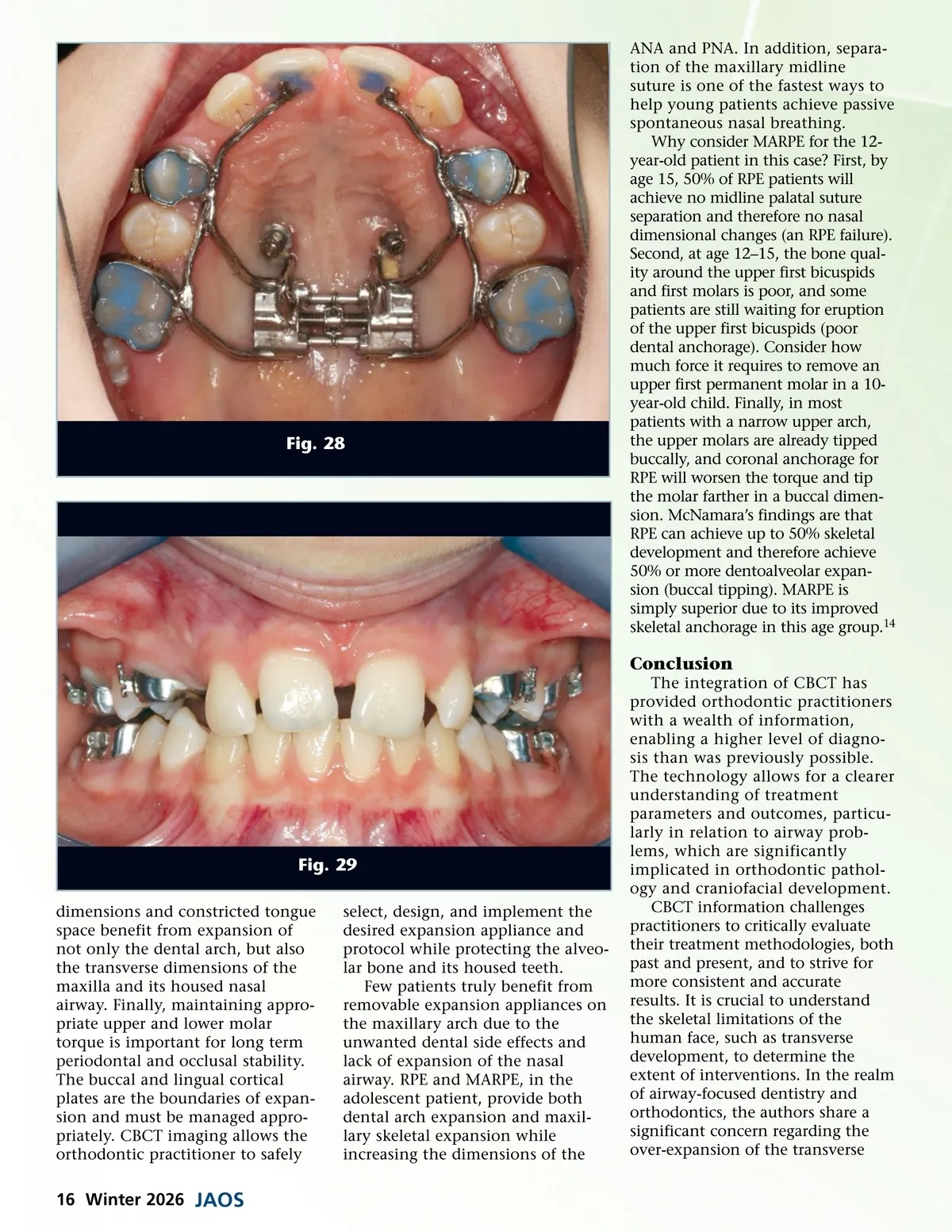
Fig. 28 ANA and PNA. In addition, separa-tion of the maxillary midline suture is one of the fastest ways to help young patients achieve passive spontaneous nasal breathing. Why consider MARPE for the 12-year-old patient in this case? First, by age 15, 50% of RPE patients will achieve no midline palatal suture separation and therefore no nasal dimensional changes (an RPE failure). Second, at age 12–15, the bone qual-ity around the upper first bicuspids and first molars is poor, and some patients are still waiting for eruption of the upper first bicuspids (poor dental anchorage). Consider how much force it requires to remove an upper first permanent molar in a 10-year-old child. Finally, in most patients with a narrow upper arch, the upper molars are already tipped buccally, and coronal anchorage for RPE will worsen the torque and tip the molar farther in a buccal dimen-sion. McNamara’s findings are that RPE can achieve up to 50% skeletal development and therefore achieve 50% or more dentoalveolar expan-sion (buccal tipping). MARPE is simply superior due to its improved skeletal anchorage in this age group. 14 Conclusion The integration of CBCT has provided orthodontic practitioners with a wealth of information, enabling a higher level of diagno-sis than was previously possible. The technology allows for a clearer understanding of treatment parameters and outcomes, particu-larly in relation to airway prob-lems, which are significantly implicated in orthodontic pathol-ogy and craniofacial development. CBCT information challenges practitioners to critically evaluate their treatment methodologies, both past and present, and to strive for more consistent and accurate results. It is crucial to understand the skeletal limitations of the human face, such as transverse development, to determine the extent of interventions. In the realm of airway-focused dentistry and orthodontics, the authors share a significant concern regarding the over-expansion of the transverse Fig. 29 dimensions and constricted tongue space benefit from expansion of not only the dental arch, but also the transverse dimensions of the maxilla and its housed nasal airway. Finally, maintaining appro-priate upper and lower molar torque is important for long term periodontal and occlusal stability. The buccal and lingual cortical plates are the boundaries of expan-sion and must be managed appro-priately. CBCT imaging allows the orthodontic practitioner to safely select, design, and implement the desired expansion appliance and protocol while protecting the alveo-lar bone and its housed teeth. Few patients truly benefit from removable expansion appliances on the maxillary arch due to the unwanted dental side effects and lack of expansion of the nasal airway. RPE and MARPE, in the adolescent patient, provide both dental arch expansion and maxil-lary skeletal expansion while increasing the dimensions of the 16 Winter 2026 JAOS
Journal of the American Orthodontic Society Winter 2026: Page 16