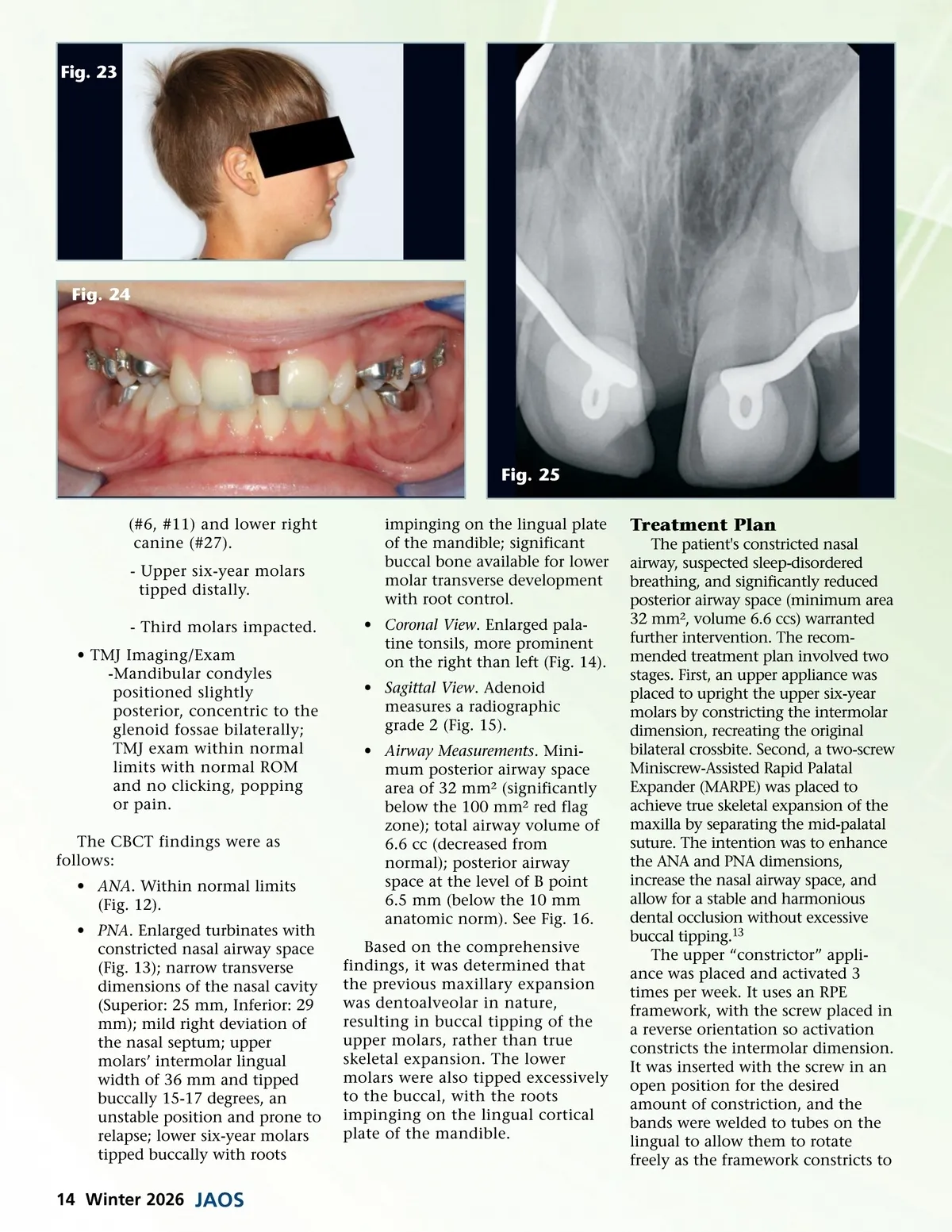
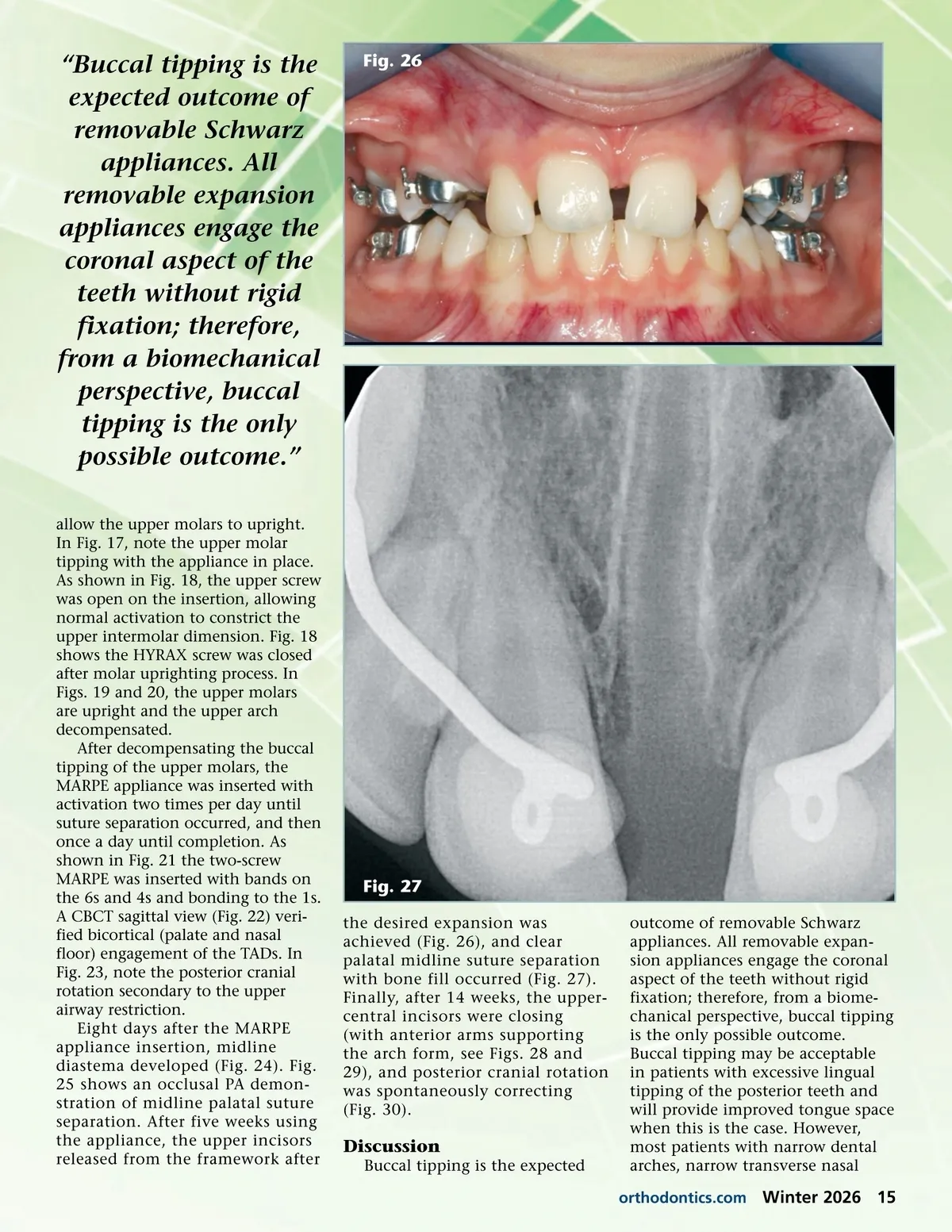
Fig. 23 Fig. 24 Fig. 25 (#6, #11) and lower right canine (#27). -Upper six-year molars tipped distally. -Third molars impacted. • TMJ Imaging/Exam -Mandibular condyles positioned slightly posterior, concentric to the glenoid fossae bilaterally; TMJ exam within normal limits with normal ROM and no clicking, popping or pain. The CBCT findings were as follows: • ANA . Within normal limits (Fig. 12). • PNA . Enlarged turbinates with constricted nasal airway space (Fig. 13); narrow transverse dimensions of the nasal cavity (Superior: 25 mm, Inferior: 29 mm); mild right deviation of the nasal septum; upper molars’ intermolar lingual width of 36 mm and tipped buccally 15-17 degrees, an unstable position and prone to relapse; lower six-year molars tipped buccally with roots impinging on the lingual plate of the mandible; significant buccal bone available for lower molar transverse development with root control. • Coronal View . Enlarged pala-tine tonsils, more prominent on the right than left (Fig. 14). • Sagittal View . Adenoid measures a radiographic grade 2 (Fig. 15). • Airway Measurements . Mini-mum posterior airway space area of 32 mm² (significantly below the 100 mm² red flag zone); total airway volume of 6.6 cc (decreased from normal); posterior airway space at the level of B point 6.5 mm (below the 10 mm anatomic norm). See Fig. 16. Based on the comprehensive findings, it was determined that the previous maxillary expansion was dentoalveolar in nature, resulting in buccal tipping of the upper molars, rather than true skeletal expansion. The lower molars were also tipped excessively to the buccal, with the roots impinging on the lingual cortical plate of the mandible. Treatment Plan The patient's constricted nasal airway, suspected sleep-disordered breathing, and significantly reduced posterior airway space (minimum area 32 mm², volume 6.6 ccs) warranted further intervention. The recom-mended treatment plan involved two stages. First, an upper appliance was placed to upright the upper six-year molars by constricting the intermolar dimension, recreating the original bilateral crossbite. Second, a two-screw Miniscrew-Assisted Rapid Palatal Expander (MARPE) was placed to achieve true skeletal expansion of the maxilla by separating the mid-palatal suture. The intention was to enhance the ANA and PNA dimensions, increase the nasal airway space, and allow for a stable and harmonious dental occlusion without excessive buccal tipping. 13 The upper “constrictor” appli-ance was placed and activated 3 times per week. It uses an RPE framework, with the screw placed in a reverse orientation so activation constricts the intermolar dimension. It was inserted with the screw in an open position for the desired amount of constriction, and the bands were welded to tubes on the lingual to allow them to rotate freely as the framework constricts to 14 Winter 2026 JAOS
Journal of the American Orthodontic Society Winter 2026: Page 14