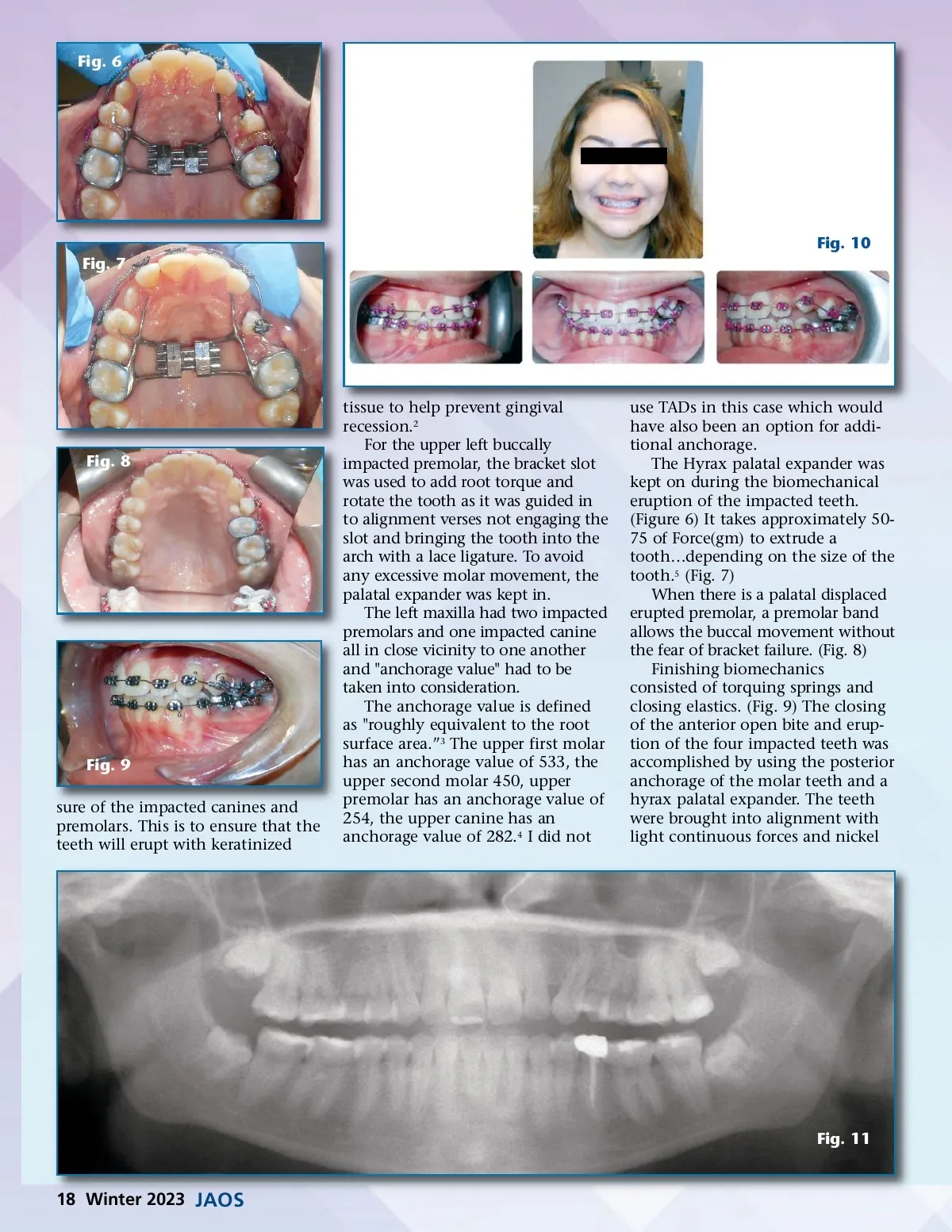
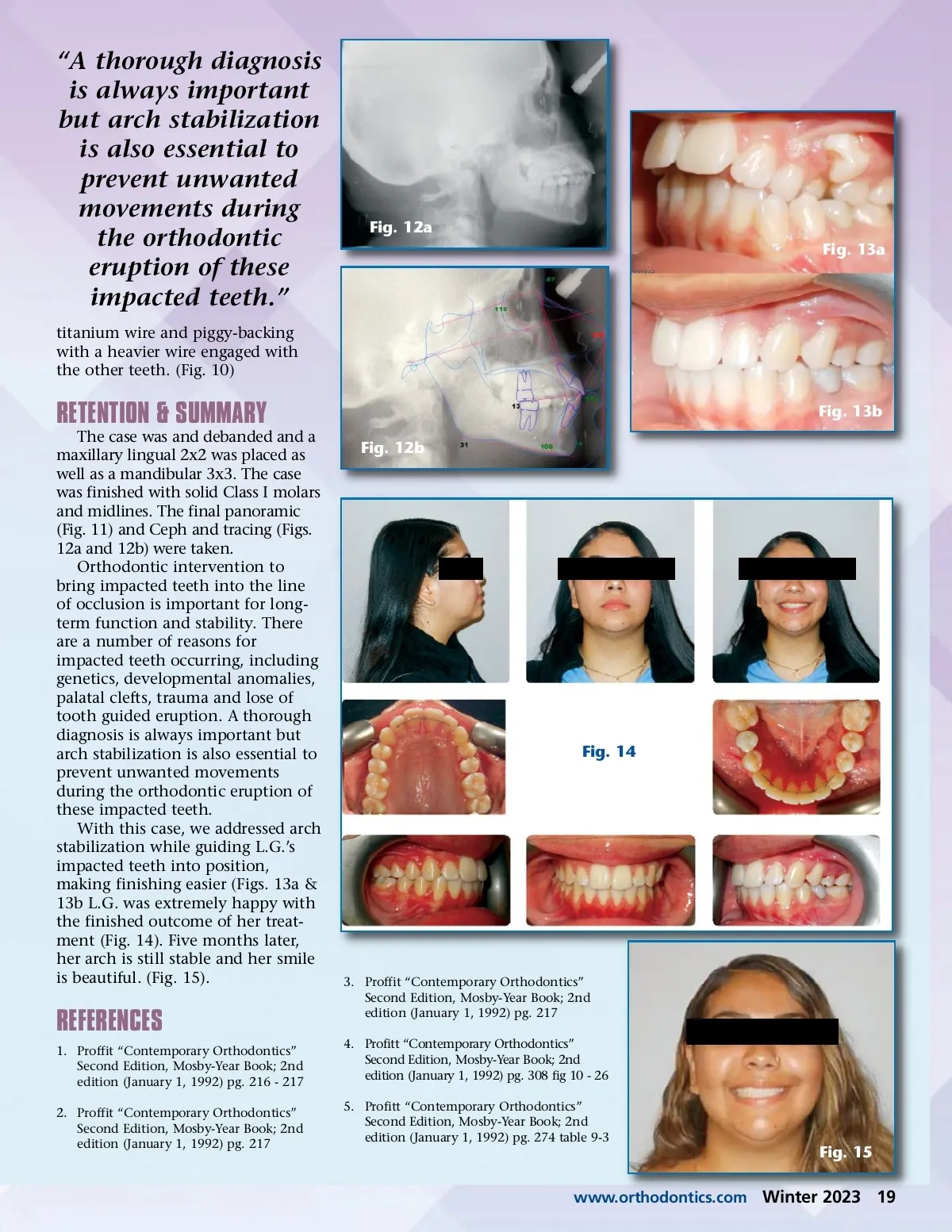
Fig. 6 Fig. 10 Fig. 7 Fig. 8 Fig. 9 sure of the impacted canines and premolars. This is to ensure that the teeth will erupt with keratinized tissue to help prevent gingival recession. 2 For the upper left buccally impacted premolar, the bracket slot was used to add root torque and rotate the tooth as it was guided in to alignment verses not engaging the slot and bringing the tooth into the arch with a lace ligature. To avoid any excessive molar movement, the palatal expander was kept in. The left maxilla had two impacted premolars and one impacted canine all in close vicinity to one another and "anchorage value" had to be taken into consideration. The anchorage value is defined as "roughly equivalent to the root surface area.” 3 The upper first molar has an anchorage value of 533, the upper second molar 450, upper premolar has an anchorage value of 254, the upper canine has an anchorage value of 282. 4 I did not use TADs in this case which would have also been an option for addi-tional anchorage. The Hyrax palatal expander was kept on during the biomechanical eruption of the impacted teeth. (Figure 6) It takes approximately 50-75 of Force(gm) to extrude a tooth…depending on the size of the tooth. 5 (Fig. 7) When there is a palatal displaced erupted premolar, a premolar band allows the buccal movement without the fear of bracket failure. (Fig. 8) Finishing biomechanics consisted of torquing springs and closing elastics. (Fig. 9) The closing of the anterior open bite and erup-tion of the four impacted teeth was accomplished by using the posterior anchorage of the molar teeth and a hyrax palatal expander. The teeth were brought into alignment with light continuous forces and nickel Fig. 11 18 Winter 2023 JAOS
Journal of the American Orthodontic Society Winter 2023: Page 18