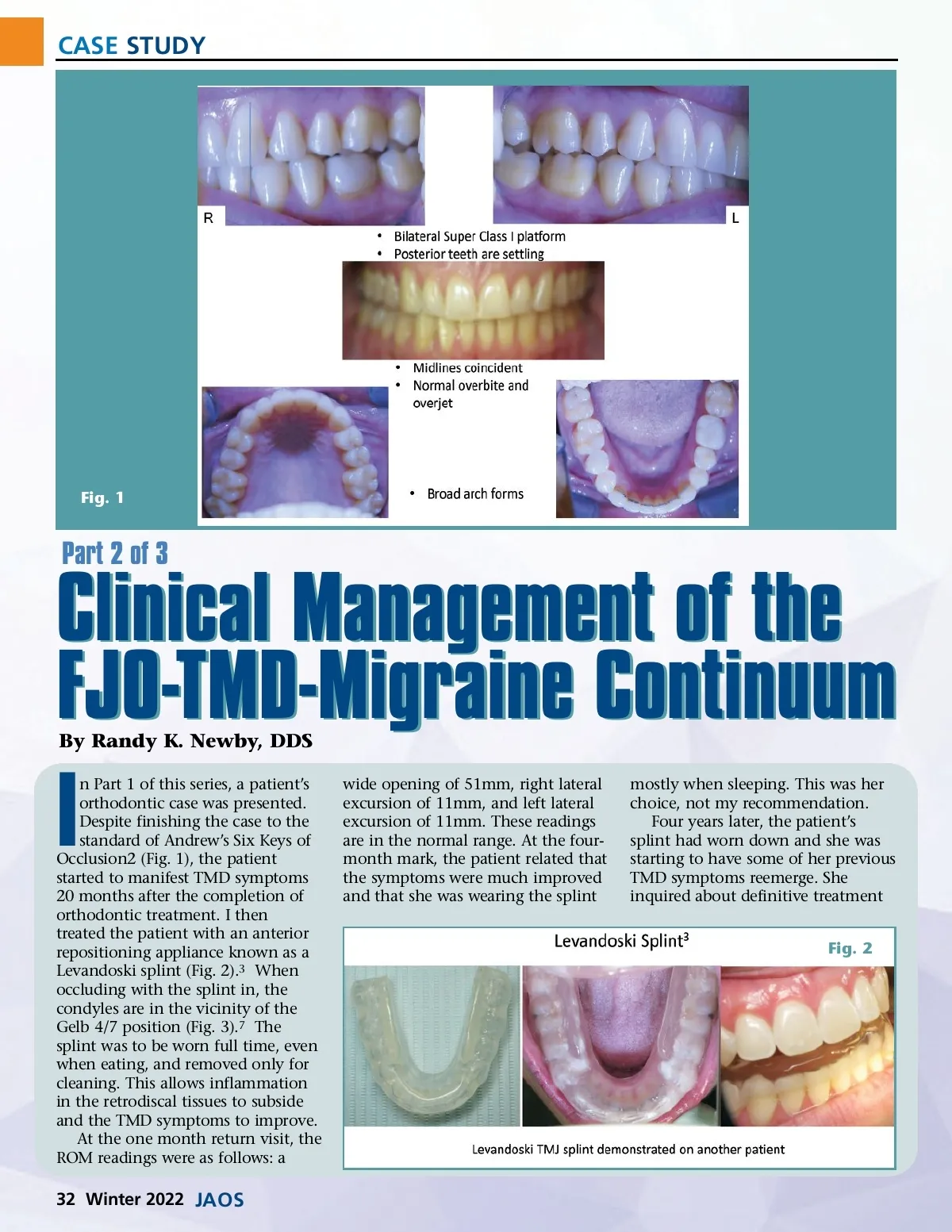
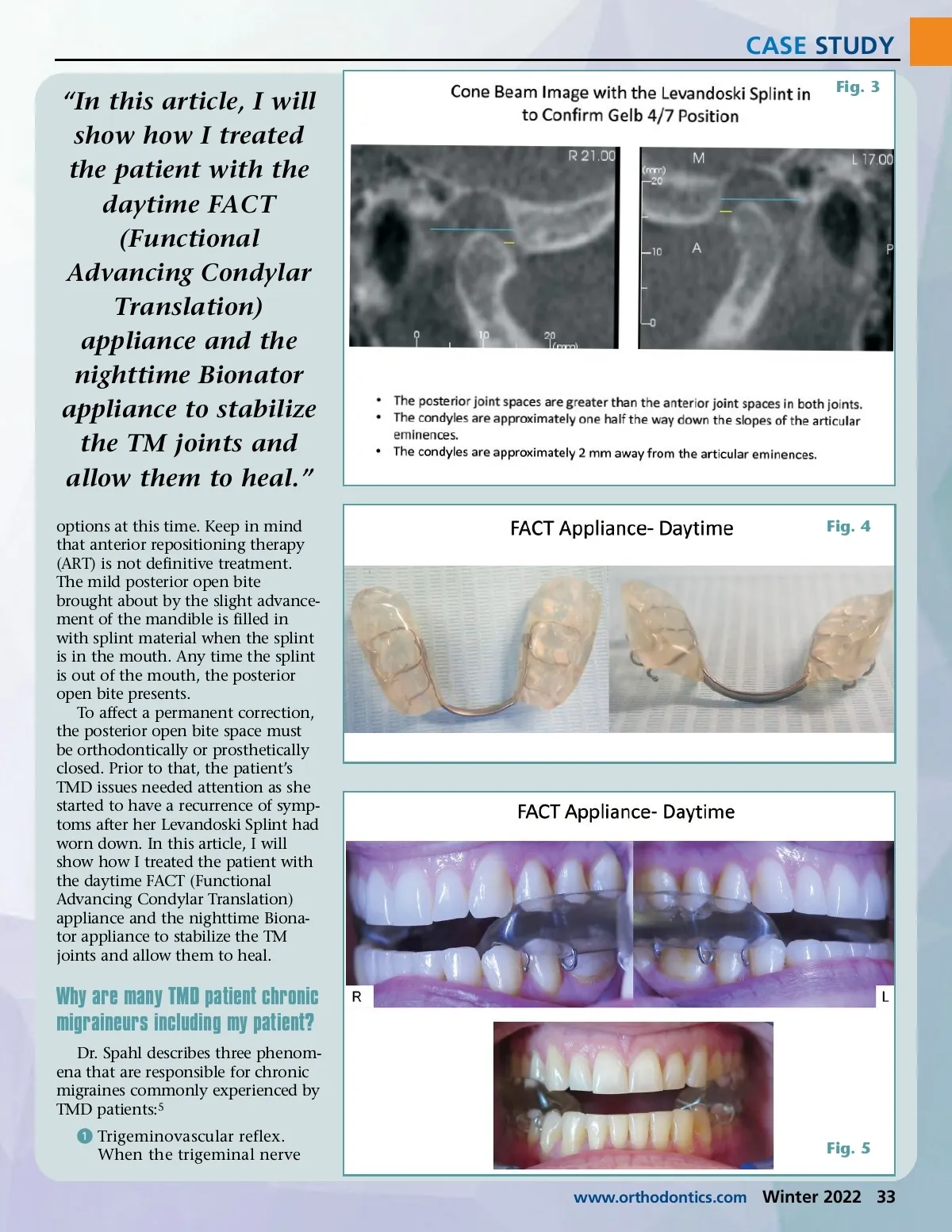
CASE STUDY Fig. 1 Part 2 of 3 Clinical Management of the FJO-TMD-Migraine Continuum By Randy K. Newby, DDS I n Part 1 of this series, a patient’s orthodontic case was presented. Despite finishing the case to the standard of Andrew’s Six Keys of Occlusion2 (Fig. 1), the patient started to manifest TMD symptoms 20 months after the completion of orthodontic treatment. I then treated the patient with an anterior repositioning appliance known as a Levandoski splint (Fig. 2). 3 When occluding with the splint in, the condyles are in the vicinity of the Gelb 4/7 position (Fig. 3). 7 The splint was to be worn full time, even when eating, and removed only for cleaning. This allows inflammation in the retrodiscal tissues to subside and the TMD symptoms to improve. At the one month return visit, the ROM readings were as follows: a wide opening of 51mm, right lateral excursion of 11mm, and left lateral excursion of 11mm. These readings are in the normal range. At the four-month mark, the patient related that the symptoms were much improved and that she was wearing the splint mostly when sleeping. This was her choice, not my recommendation. Four years later, the patient’s splint had worn down and she was starting to have some of her previous TMD symptoms reemerge. She inquired about definitive treatment Fig. 2 32 Winter 2022 JAOS
Journal of the American Orthodontic Society Winter 2022: Page 32