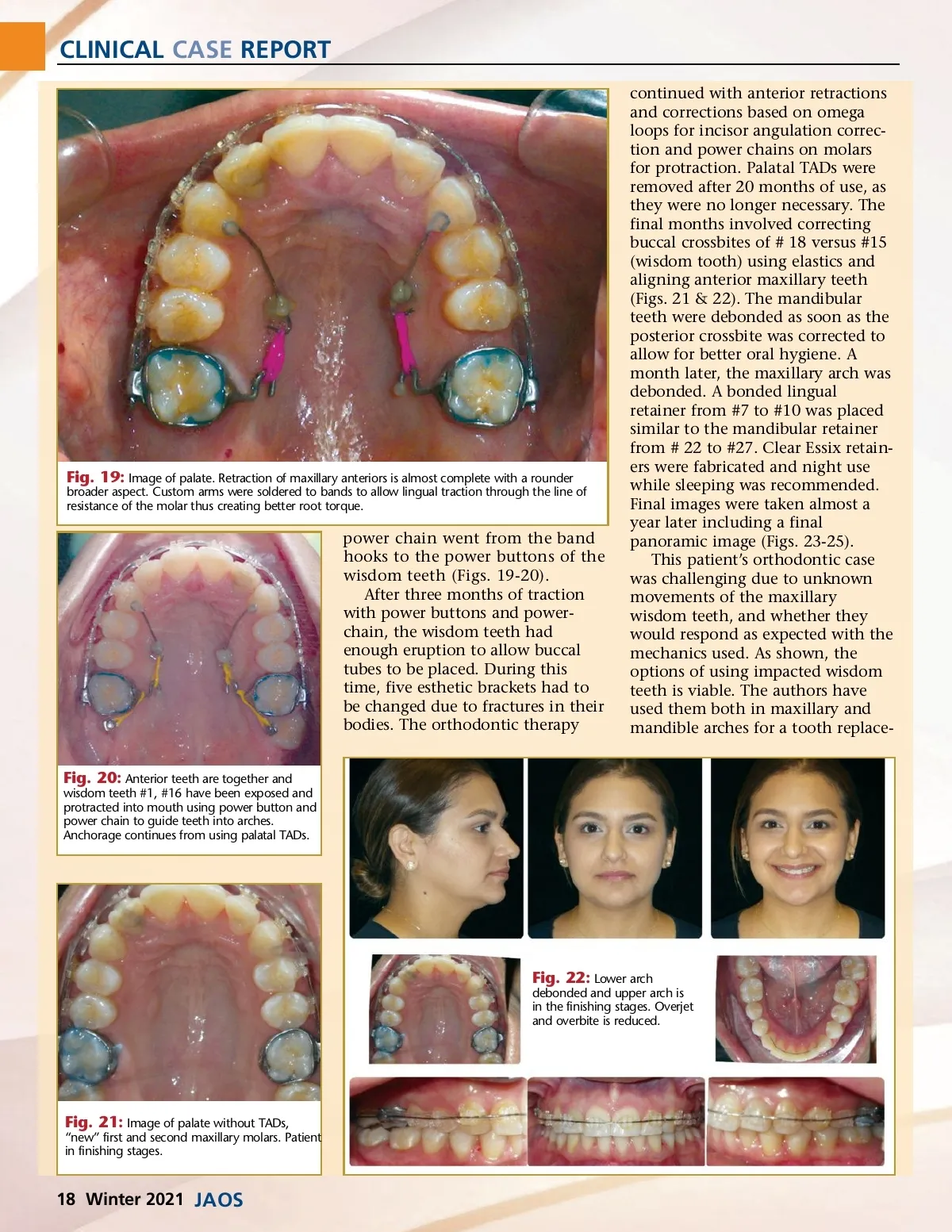
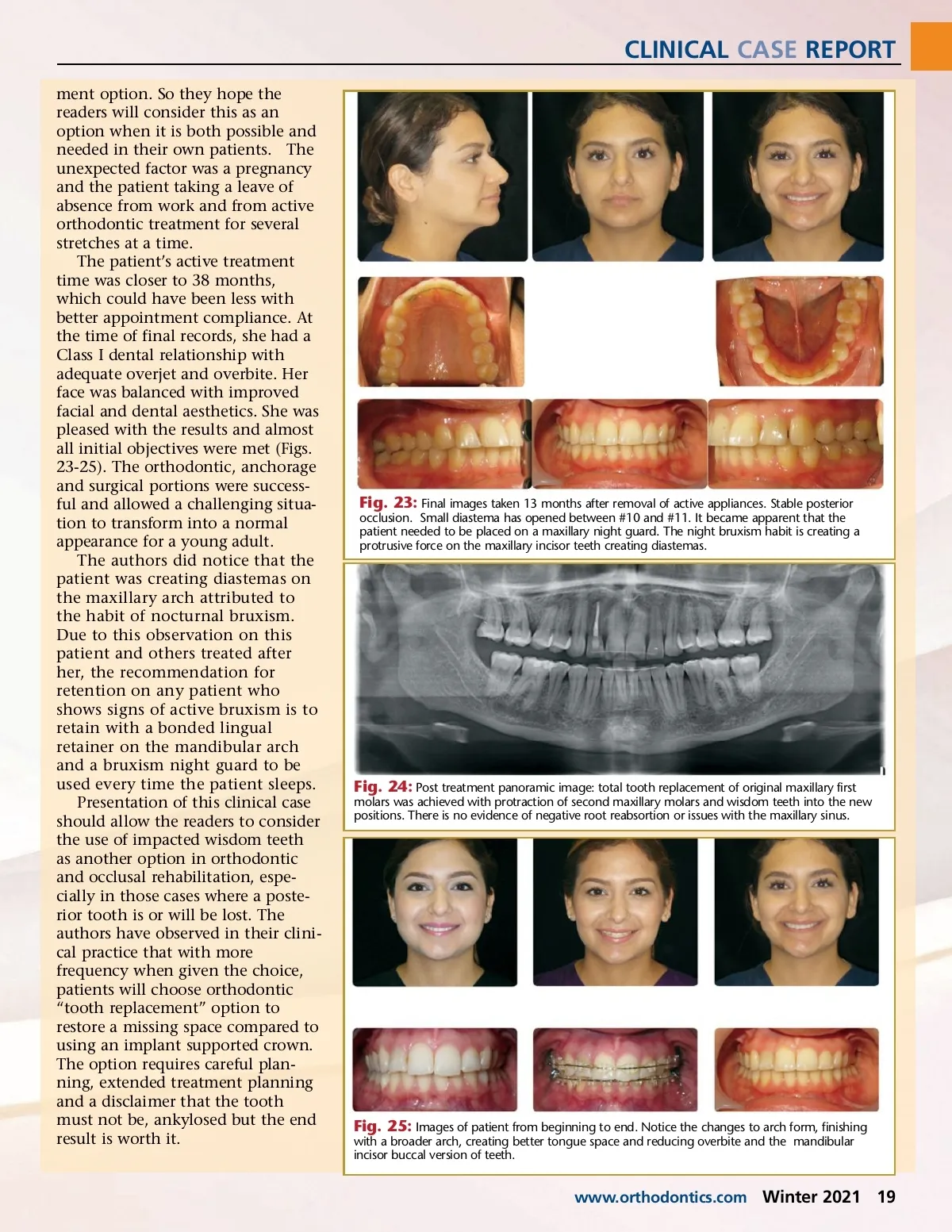
CLINICAL CASE REPORT ment option. So they hope the readers will consider this as an option when it is both possible and needed in their own patients. The unexpected factor was a pregnancy and the patient taking a leave of absence from work and from active orthodontic treatment for several stretches at a time. The patient’s active treatment time was closer to 38 months, which could have been less with better appointment compliance. At the time of final records, she had a Class I dental relationship with adequate overjet and overbite. Her face was balanced with improved facial and dental aesthetics. She was pleased with the results and almost all initial objectives were met (Figs. 23-25). The orthodontic, anchorage and surgical portions were success-ful and allowed a challenging situa-tion to transform into a normal appearance for a young adult. The authors did notice that the patient was creating diastemas on the maxillary arch attributed to the habit of nocturnal bruxism. Due to this observation on this patient and others treated after her, the recommendation for retention on any patient who shows signs of active bruxism is to retain with a bonded lingual retainer on the mandibular arch and a bruxism night guard to be used every time the patient sleeps. Presentation of this clinical case should allow the readers to consider the use of impacted wisdom teeth as another option in orthodontic and occlusal rehabilitation, espe-cially in those cases where a poste-rior tooth is or will be lost. The authors have observed in their clini-cal practice that with more frequency when given the choice, patients will choose orthodontic “tooth replacement” option to restore a missing space compared to using an implant supported crown. The option requires careful plan-ning, extended treatment planning and a disclaimer that the tooth must not be, ankylosed but the end result is worth it. Fig. 23: Final images taken 13 months after removal of active appliances. Stable posterior occlusion. Small diastema has opened between #10 and #11. It became apparent that the patient needed to be placed on a maxillary night guard. The night bruxism habit is creating a protrusive force on the maxillary incisor teeth creating diastemas. Fig. 24: Post treatment panoramic image: total tooth replacement of original maxillary first molars was achieved with protraction of second maxillary molars and wisdom teeth into the new positions. There is no evidence of negative root reabsortion or issues with the maxillary sinus. Fig. 25: Images of patient from beginning to end. Notice the changes to arch form, finishing with a broader arch, creating better tongue space and reducing overbite and the mandibular incisor buccal version of teeth. www.orthodontics.com Winter 2021 19
Journal of the American Orthodontic Society Winter 2021: Page 19