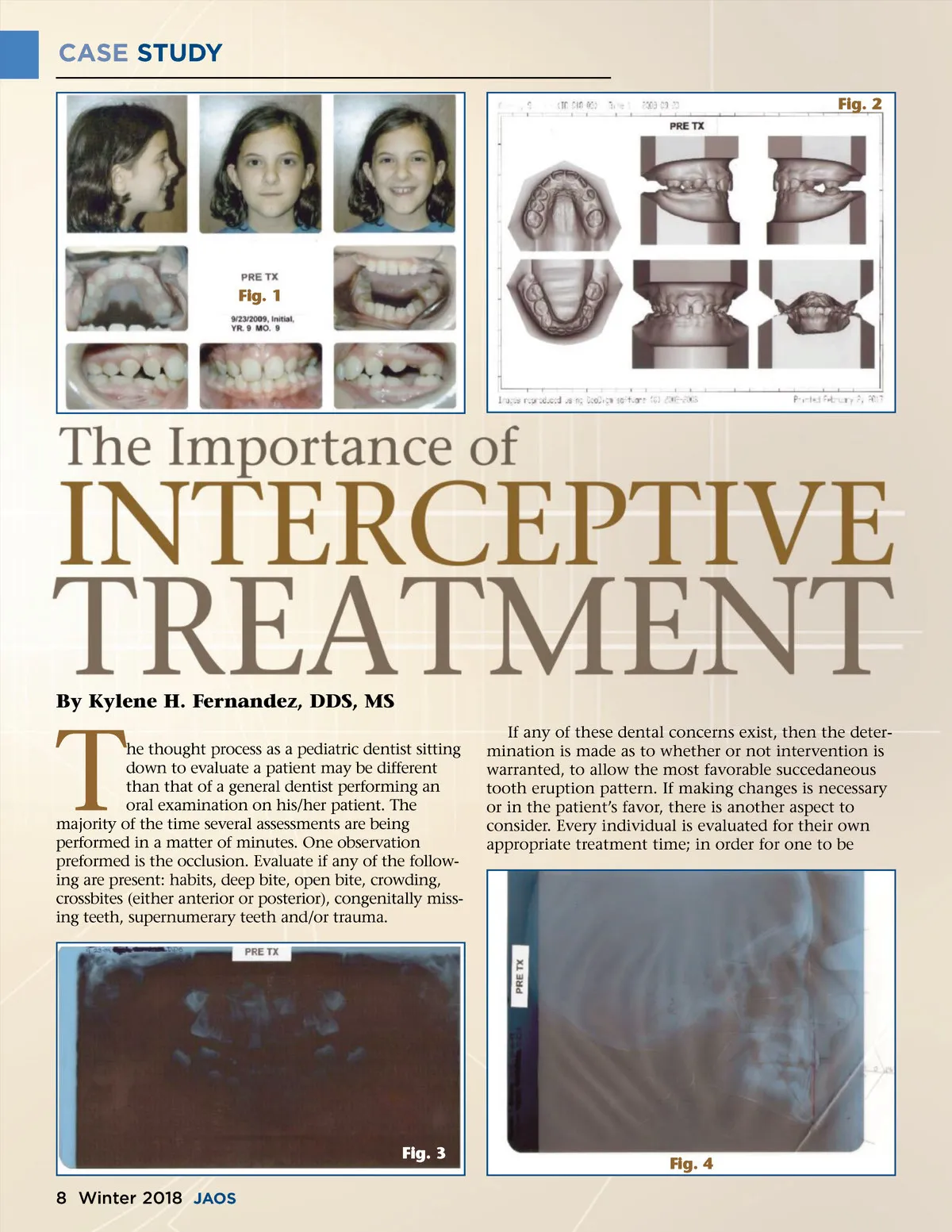
CASE STUDY “Knowing when to treat for the most favorable and most acceptable treatment experience should be a priority. Starting slowly, or at an age a little later than optimal but still prior to full permanent dentition eruption, can be very beneficial. By intervening and developing the maxillary and mandibular arches, the percentage of multiple permanent teeth extractions is greatly reduced.” ready for treatment look at the dental age, chronologi-cal age, and then just as importantly, the psychological age. Chronologic and dental ages can be similar in many patients; however, psychological age varies vastly between patients. Knowing when to treat for the most favorable and most acceptable treatment experience should be a priority. Starting slowly, or at an age a little later than optimal but still prior to full permanent dentition eruption, can be very beneficial. Interceptive orthodontics, early treatment or Phase I treatment are all names for the same orthodontic care. The main goal is to provide assistance in creating dental arches that are able to accommodate all the permanent teeth once they erupt. By intervening and developing the maxillary and mandibular arches, the percentage of multiple permanent tooth extractions is greatly reduced. The esthetic lip line or profile will end up fuller and, as time goes by, a much more favorable look for the patient will result. The following case demonstrates the benefits of beginning Phase I orthodontics at a slightly later dental age and chronologic age due to the patient’s psychological age not being ready. This patient’s treat-ment continued to a complete Phase II avoiding any extractions even though all four permanent cuspids were blocked out. sion on both the right and left sides, and her lower incisors are lingually inclined. She had premature loss of several primary teeth prior to becoming a patient in my practice and no preventative space maintainers had been placed. Her overjet is 1mm and her overbite is 7mm. She has a concave profile, and her airway appears to be normal and she has no oral habits.(Fig.1 and Fig.2) Radiographic Analysis The panoramic radiograph reveals blocked out cuspids #’s 6, 11, 22, 27. She experienced premature loss of several primary teeth. Tooth #’s 19, 30 are mesially inclined. Her maxillary and mandibular incisors are spaced and flared as “flowers in a vase.” She has imma-ture root development on maxillary premolars that have begun to erupt. Her bone density appears normal and although some of her premolars are erupting, the root formation at this point is appropriate for her age. The cephalometric radiograph was traced by hand using the method taught by Dr. Carapezza in his comprehensive early treatment courses. S.K. had a Class I skeletal classification with an ANB of 3 degrees. Her SNA measured 79 degrees and SNB was 76 degrees, both are retruded in their A-P positions. Her mandibular plane angle measured 34 degrees and had a Y-axis of 68 degrees indicating a neutral growth pattern but with the tendency towards an open vertical growth pattern. At her young age, she has 3-4 mm of potential pogonion growth. Her pogonion to NB line measured 2 mm and lower incisor to NB is 3mm. With the potential pogonion growth her lower incisors have room to come forward. With advancement of the maxilla and pogonion growth her esthetic soft tissue profile can be improved. (Fig.3 and Fig.4) Treatment Objectives: ᕡ Increase the width of the maxilla ᕢ Advance the premaxilla (A point) ᕣ Create space for blocked out cuspids ᕤ Flatten her curve of spee ᕥ Finish to Class I ᕦ Improve the patients profile and esthetic line Treatment Plan ᕡ NPE (Nitanium Palatal Expander) ᕢ UAW (Utility Arch Wire) ᕣ Create space for #6, #11, #22, #27 ᕤ Upright lower first permanent molars ᕥ Continue to bracket/bond as permanent teeth erupt ᕦ Serial guidance if necessary ᕧ Straightwire appliances www.orthodontics.com Clinical Analysis S.K. is a 9-year, 9-month old Caucasian female. She presents with blocked out teeth, bilateral crossbites, moderate curve of spee and lower first permanent molars mesially inclined. She has a Class II malocclu-Winter 2018 9
Journal of the American Orthodontic Society Winter 2018: Page 9