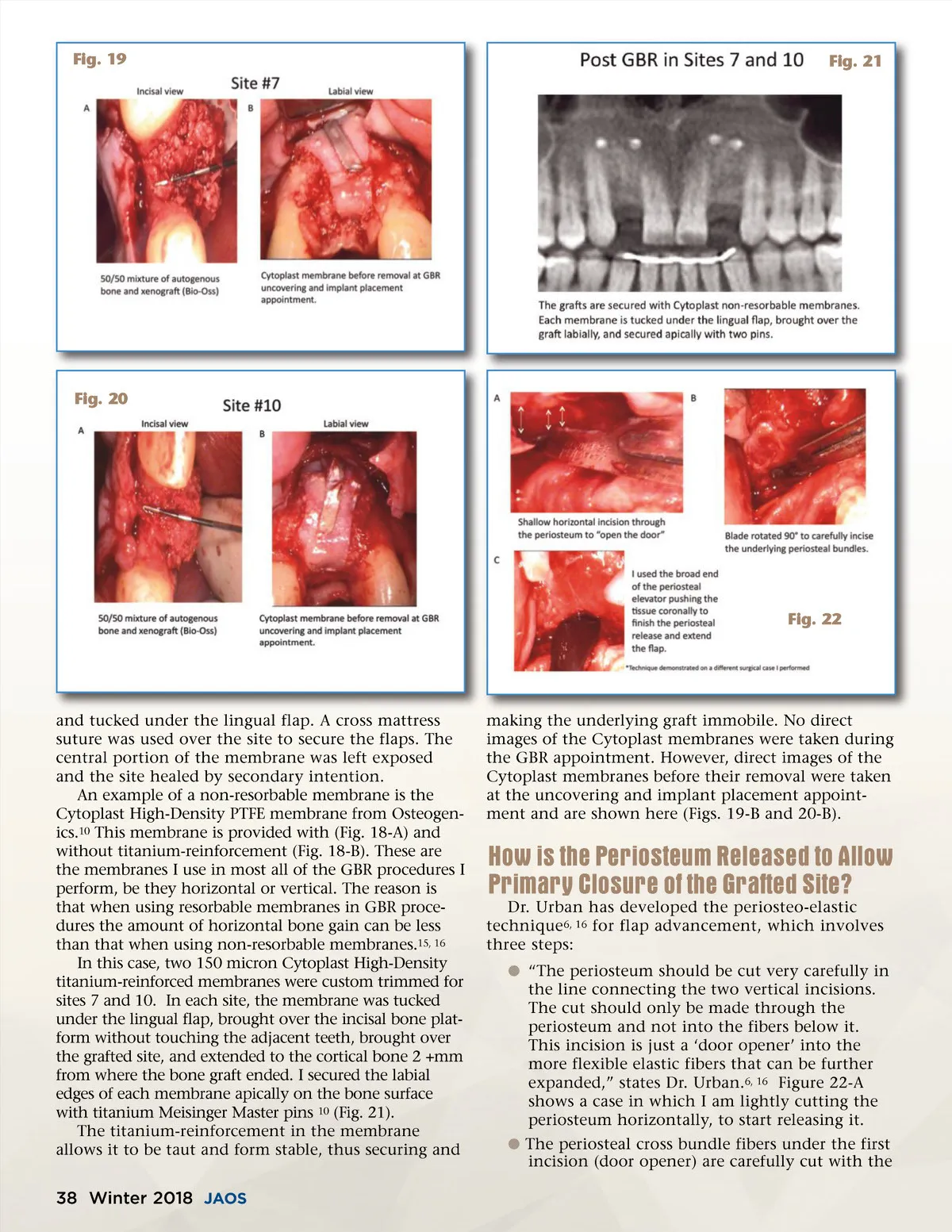
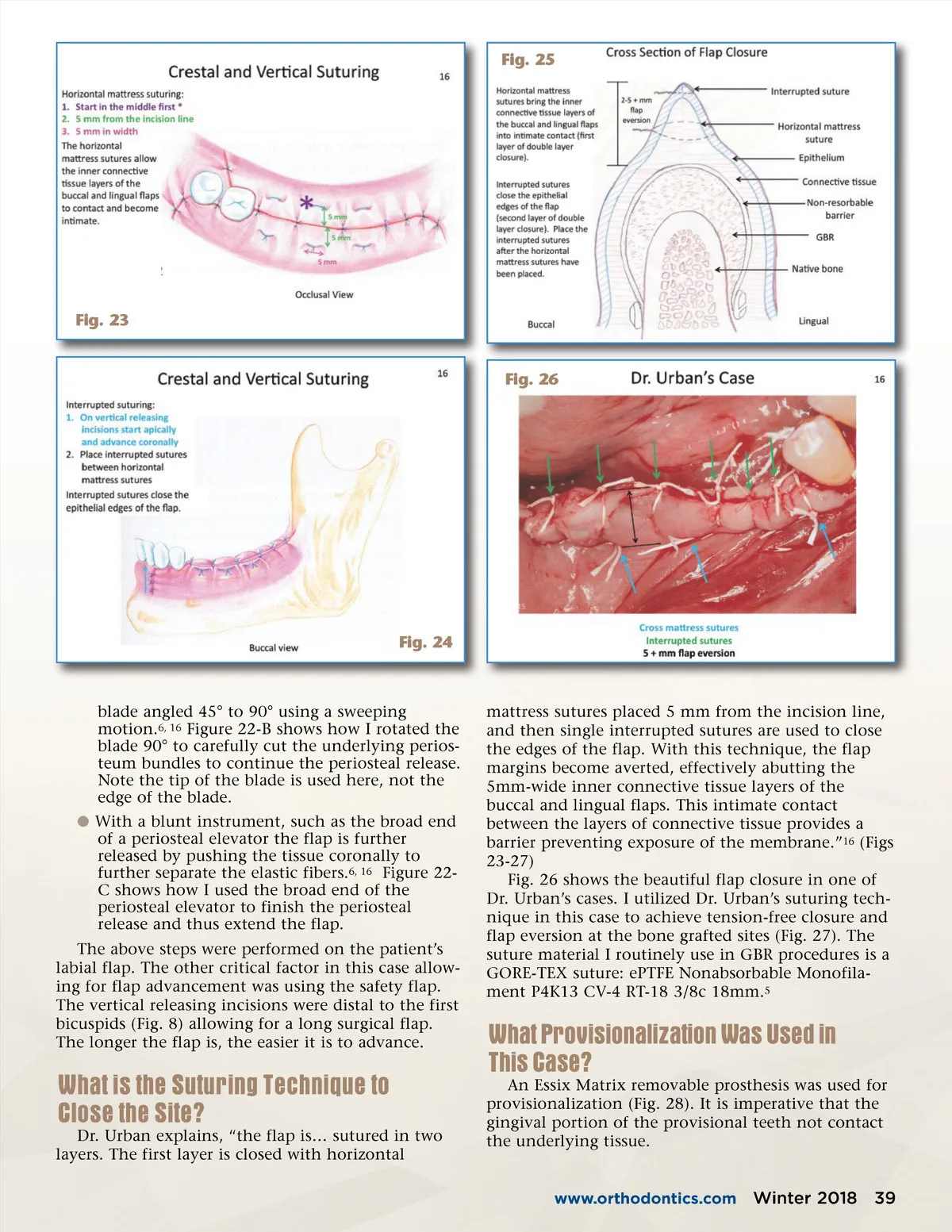
Fig. 19 Fig. 21 Fig. 20 Fig. 22 and tucked under the lingual flap. A cross mattress suture was used over the site to secure the flaps. The central portion of the membrane was left exposed and the site healed by secondary intention. An example of a non-resorbable membrane is the Cytoplast High-Density PTFE membrane from Osteogen-ics. 10 This membrane is provided with (Fig. 18-A) and without titanium-reinforcement (Fig. 18-B). These are the membranes I use in most all of the GBR procedures I perform, be they horizontal or vertical. The reason is that when using resorbable membranes in GBR proce-dures the amount of horizontal bone gain can be less than that when using non-resorbable membranes. 15, 16 In this case, two 150 micron Cytoplast High-Density titanium-reinforced membranes were custom trimmed for sites 7 and 10. In each site, the membrane was tucked under the lingual flap, brought over the incisal bone plat-form without touching the adjacent teeth, brought over the grafted site, and extended to the cortical bone 2 +mm from where the bone graft ended. I secured the labial edges of each membrane apically on the bone surface with titanium Meisinger Master pins 10 (Fig. 21). The titanium-reinforcement in the membrane allows it to be taut and form stable, thus securing and making the underlying graft immobile. No direct images of the Cytoplast membranes were taken during the GBR appointment. However, direct images of the Cytoplast membranes before their removal were taken at the uncovering and implant placement appoint-ment and are shown here (Figs. 19-B and 20-B). How is the Periosteum Released to Allow Primary Closure of the Grafted Site? Dr. Urban has developed the periosteo-elastic technique 6, 16 for flap advancement, which involves three steps: b “The periosteum should be cut very carefully in the line connecting the two vertical incisions. The cut should only be made through the periosteum and not into the fibers below it. This incision is just a ‘door opener’ into the more flexible elastic fibers that can be further expanded,” states Dr. Urban. 6, 16 Figure 22-A shows a case in which I am lightly cutting the periosteum horizontally, to start releasing it. b The periosteal cross bundle fibers under the first incision (door opener) are carefully cut with the 38 Winter 2018 JAOS
Journal of the American Orthodontic Society Winter 2018: Page 38