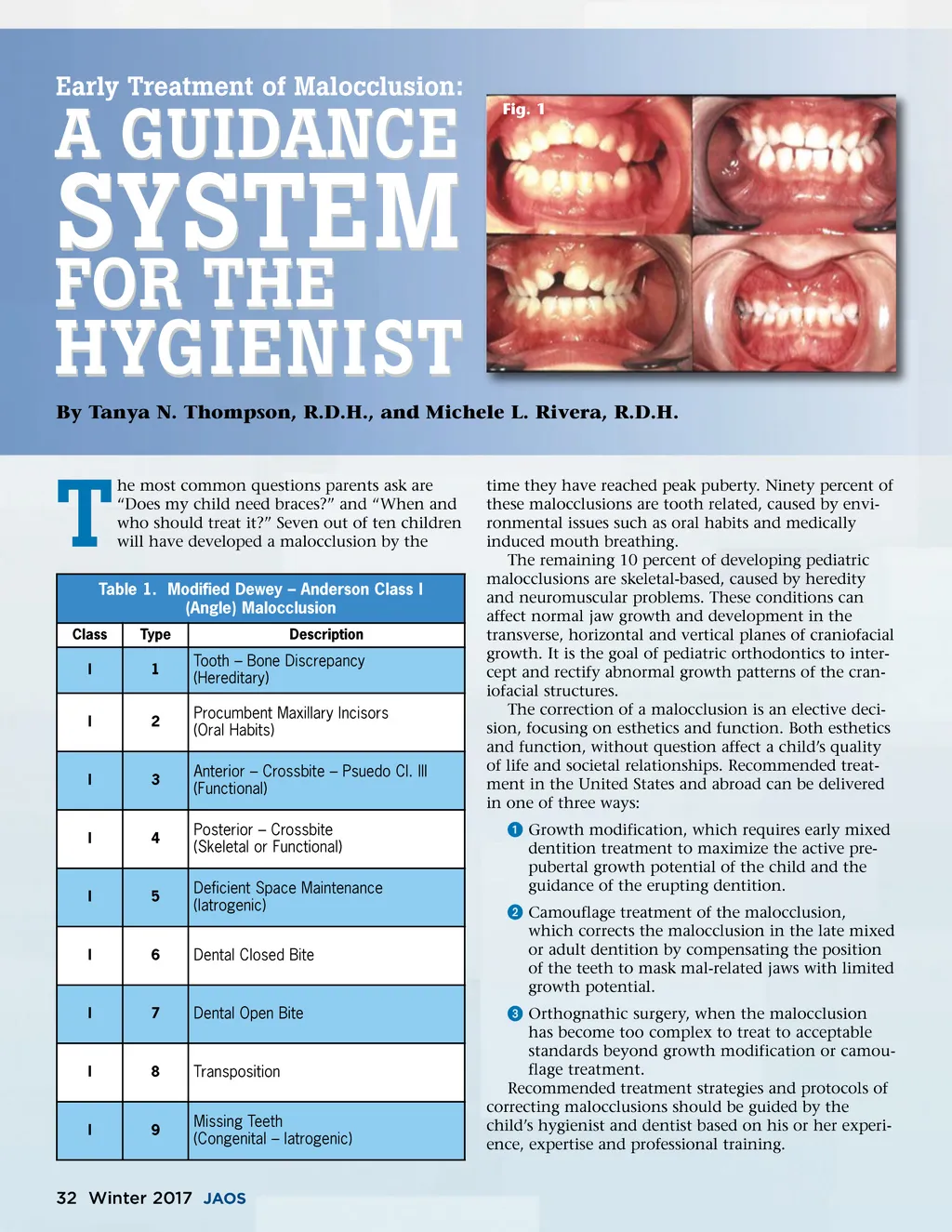
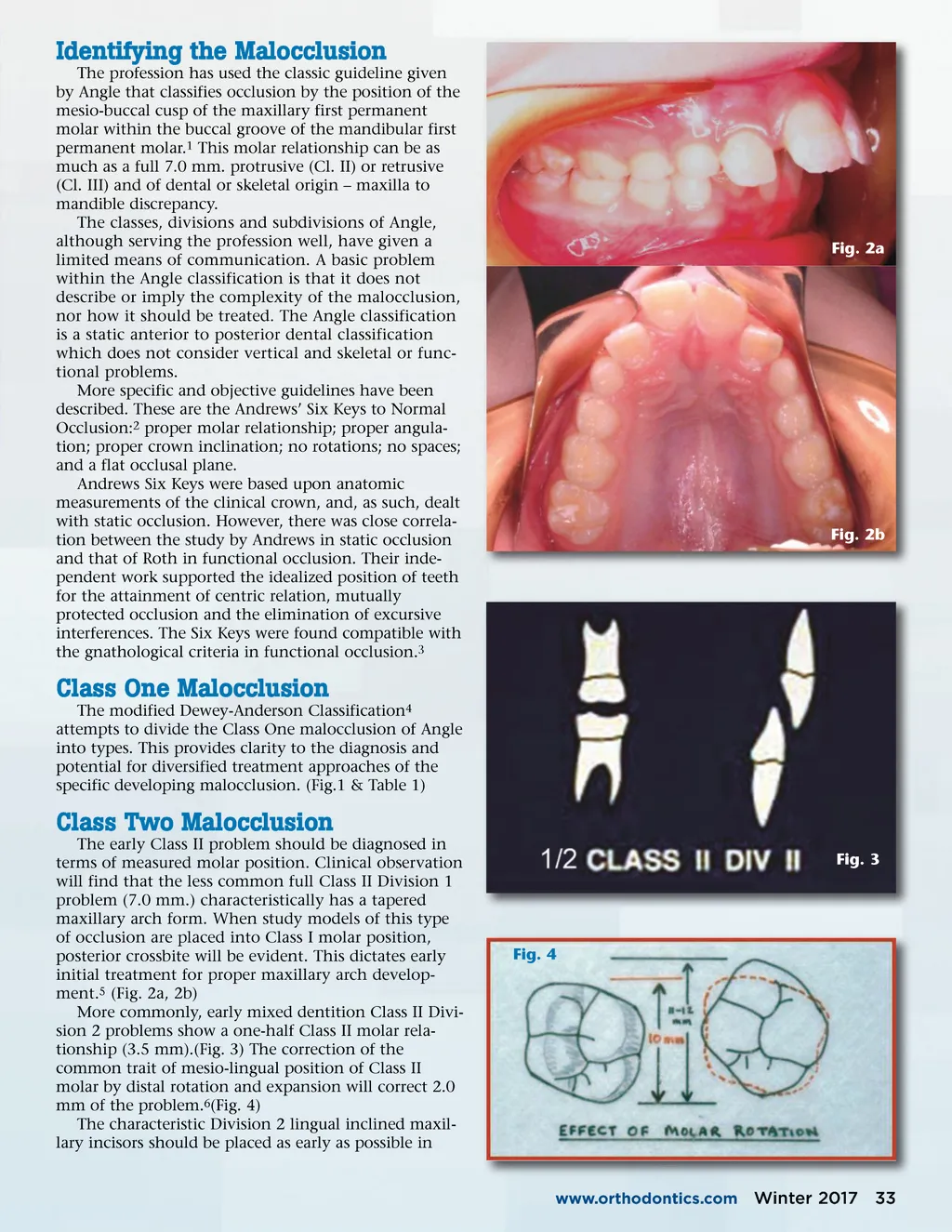
Identifying the Malocclusion The profession has used the classic guideline given by Angle that classifies occlusion by the position of the mesio-buccal cusp of the maxillary first permanent molar within the buccal groove of the mandibular first permanent molar. 1 This molar relationship can be as much as a full 7.0 mm. protrusive (Cl. II) or retrusive (Cl. III) and of dental or skeletal origin – maxilla to mandible discrepancy. The classes, divisions and subdivisions of Angle, although serving the profession well, have given a limited means of communication. A basic problem within the Angle classification is that it does not describe or imply the complexity of the malocclusion, nor how it should be treated. The Angle classification is a static anterior to posterior dental classification which does not consider vertical and skeletal or func-tional problems. More specific and objective guidelines have been described. These are the Andrews’ Six Keys to Normal Occlusion: 2 proper molar relationship; proper angula-tion; proper crown inclination; no rotations; no spaces; and a flat occlusal plane. Andrews Six Keys were based upon anatomic measurements of the clinical crown, and, as such, dealt with static occlusion. However, there was close correla-tion between the study by Andrews in static occlusion and that of Roth in functional occlusion. Their inde-pendent work supported the idealized position of teeth for the attainment of centric relation, mutually protected occlusion and the elimination of excursive interferences. The Six Keys were found compatible with the gnathological criteria in functional occlusion. 3 Fig. 2a Fig. 2b Class One Malocclusion The modified Dewey-Anderson Classification 4 attempts to divide the Class One malocclusion of Angle into types. This provides clarity to the diagnosis and potential for diversified treatment approaches of the specific developing malocclusion. (Fig.1 & Table 1) Class Two Malocclusion The early Class II problem should be diagnosed in terms of measured molar position. Clinical observation will find that the less common full Class II Division 1 problem (7.0 mm.) characteristically has a tapered maxillary arch form. When study models of this type of occlusion are placed into Class I molar position, posterior crossbite will be evident. This dictates early initial treatment for proper maxillary arch develop-ment. 5 (Fig. 2a, 2b) More commonly, early mixed dentition Class II Divi-sion 2 problems show a one-half Class II molar rela-tionship (3.5 mm).(Fig. 3) The correction of the common trait of mesio-lingual position of Class II molar by distal rotation and expansion will correct 2.0 mm of the problem. 6 (Fig. 4) The characteristic Division 2 lingual inclined maxil-lary incisors should be placed as early as possible in Fig. 3 Fig. 4 www.orthodontics.com Winter 2017 33
Journal of the American Orthodontic Society Winter 2017: Page 33