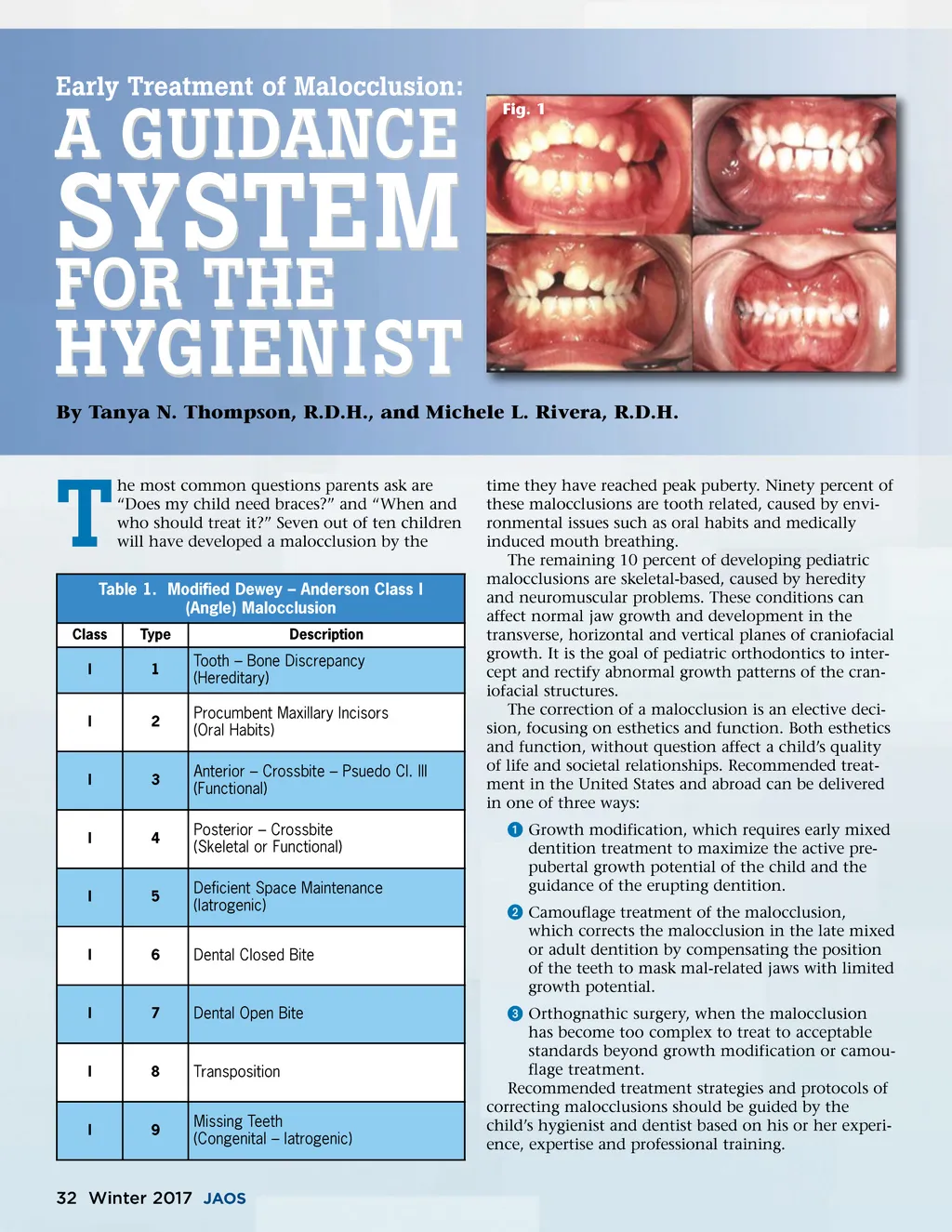
Early Treatment of Malocclusion: SYSTEM FOR THE A GUIDANCE Fig. 1 HYGIENIST By Tanya N. Thompson, R.D.H., and Michele L. Rivera, R.D.H. T Class I I I he most common questions parents ask are “Does my child need braces?” and “When and who should treat it?” Seven out of ten children will have developed a malocclusion by the Table 1. Modified Dewey – Anderson Class I (Angle) Malocclusion Type 1 Description Tooth – Bone Discrepancy (Hereditary) Procumbent Maxillary Incisors (Oral Habits) Anterior – Crossbite – Psuedo Cl. III (Functional) Posterior – Crossbite (Skeletal or Functional) Deficient Space Maintenance (Iatrogenic) Dental Closed Bite 2 3 time they have reached peak puberty. Ninety percent of these malocclusions are tooth related, caused by envi-ronmental issues such as oral habits and medically induced mouth breathing. The remaining 10 percent of developing pediatric malocclusions are skeletal-based, caused by heredity and neuromuscular problems. These conditions can affect normal jaw growth and development in the transverse, horizontal and vertical planes of craniofacial growth. It is the goal of pediatric orthodontics to inter-cept and rectify abnormal growth patterns of the cran-iofacial structures. The correction of a malocclusion is an elective deci-sion, focusing on esthetics and function. Both esthetics and function, without question affect a child’s quality of life and societal relationships. Recommended treat-ment in the United States and abroad can be delivered in one of three ways: ᕡ Growth modification, which requires early mixed dentition treatment to maximize the active pre-pubertal growth potential of the child and the guidance of the erupting dentition. ᕢ Camouflage treatment of the malocclusion, which corrects the malocclusion in the late mixed or adult dentition by compensating the position of the teeth to mask mal-related jaws with limited growth potential. ᕣ Orthognathic surgery, when the malocclusion has become too complex to treat to acceptable standards beyond growth modification or camou-flage treatment. Recommended treatment strategies and protocols of correcting malocclusions should be guided by the child’s hygienist and dentist based on his or her experi-ence, expertise and professional training. I 4 I 5 I 6 I 7 Dental Open Bite I 8 Transposition Missing Teeth (Congenital – Iatrogenic) I 9 32 Winter 2017 JAOS
Journal of the American Orthodontic Society Winter 2017: Page 32