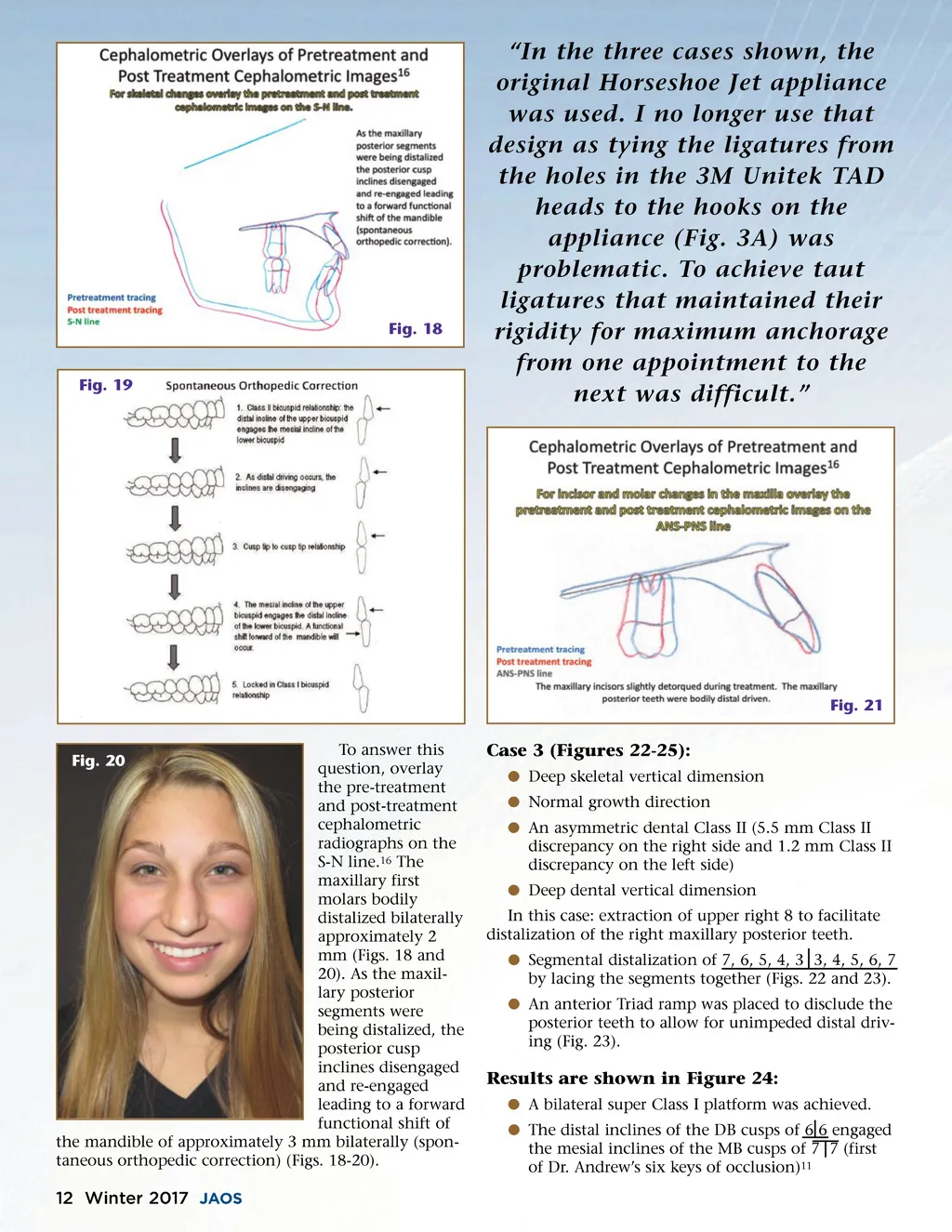
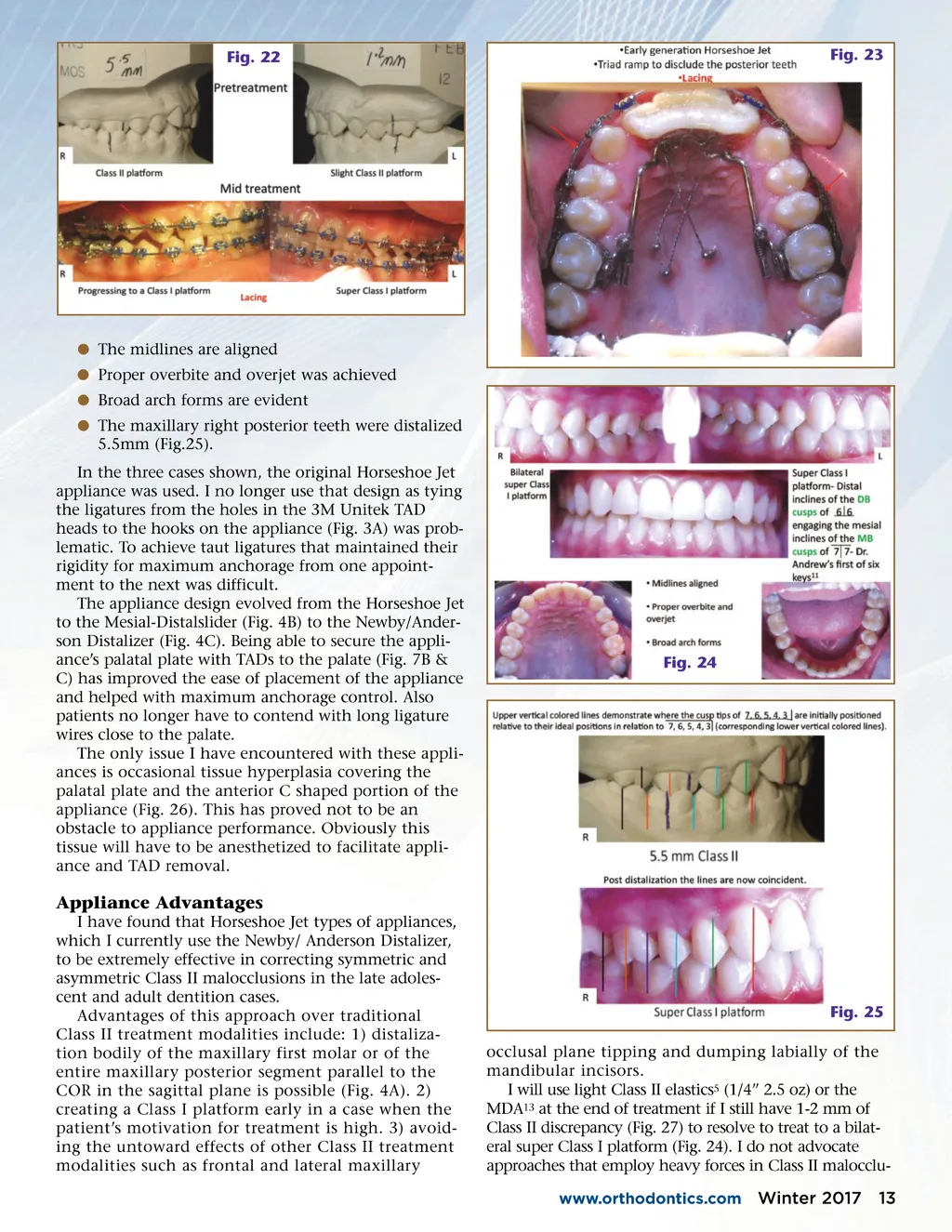
Fig. 22 Fig. 23 b The midlines are aligned b Proper overbite and overjet was achieved b Broad arch forms are evident b The maxillary right posterior teeth were distalized 5.5mm (Fig.25). In the three cases shown, the original Horseshoe Jet appliance was used. I no longer use that design as tying the ligatures from the holes in the 3M Unitek TAD heads to the hooks on the appliance (Fig. 3A) was prob-lematic. To achieve taut ligatures that maintained their rigidity for maximum anchorage from one appoint-ment to the next was difficult. The appliance design evolved from the Horseshoe Jet to the Mesial-Distalslider (Fig. 4B) to the Newby/Ander-son Distalizer (Fig. 4C). Being able to secure the appli-ance’s palatal plate with TADs to the palate (Fig. 7B & C) has improved the ease of placement of the appliance and helped with maximum anchorage control. Also patients no longer have to contend with long ligature wires close to the palate. The only issue I have encountered with these appli-ances is occasional tissue hyperplasia covering the palatal plate and the anterior C shaped portion of the appliance (Fig. 26). This has proved not to be an obstacle to appliance performance. Obviously this tissue will have to be anesthetized to facilitate appli-ance and TAD removal. Fig. 24 Appliance Advantages I have found that Horseshoe Jet types of appliances, which I currently use the Newby/ Anderson Distalizer, to be extremely effective in correcting symmetric and asymmetric Class II malocclusions in the late adoles-cent and adult dentition cases. Advantages of this approach over traditional Class II treatment modalities include: 1) distaliza-tion bodily of the maxillary first molar or of the entire maxillary posterior segment parallel to the COR in the sagittal plane is possible (Fig. 4A). 2) creating a Class I platform early in a case when the patient’s motivation for treatment is high. 3) avoid-ing the untoward effects of other Class II treatment modalities such as frontal and lateral maxillary Fig. 25 occlusal plane tipping and dumping labially of the mandibular incisors. I will use light Class II elastics 5 (1/4” 2.5 oz) or the MDA 13 at the end of treatment if I still have 1-2 mm of Class II discrepancy (Fig. 27) to resolve to treat to a bilat-eral super Class I platform (Fig. 24). I do not advocate approaches that employ heavy forces in Class II malocclu-www.orthodontics.com Winter 2017 13
Journal of the American Orthodontic Society Winter 2017: Page 13