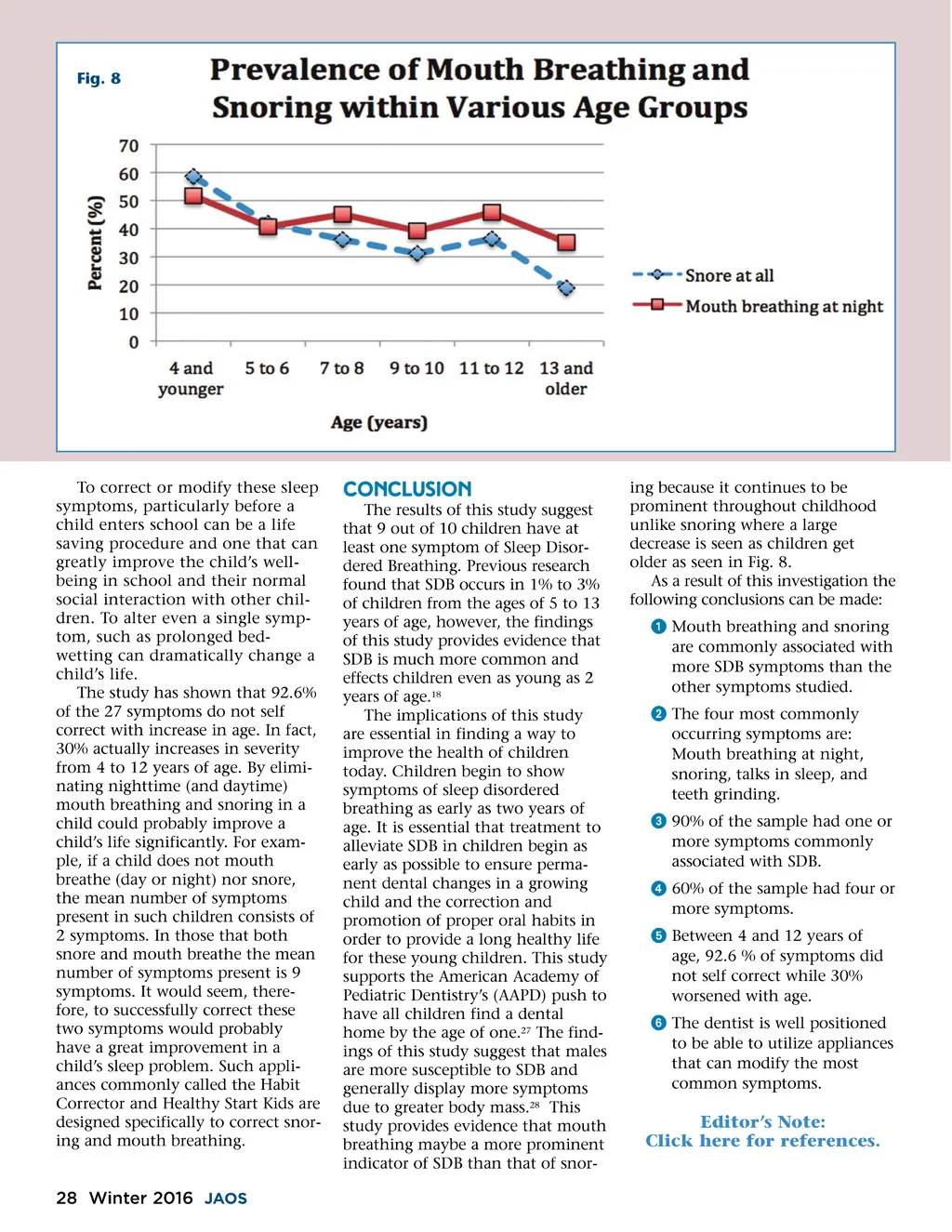
Fig. 8 To correct or modify these sleep symptoms, particularly before a child enters school can be a life saving procedure and one that can greatly improve the child’s well-being in school and their normal social interaction with other chil-dren. To alter even a single symp-tom, such as prolonged bed-wetting can dramatically change a child’s life. The study has shown that 92.6% of the 27 symptoms do not self correct with increase in age. In fact, 30% actually increases in severity from 4 to 12 years of age. By elimi-nating nighttime (and daytime) mouth breathing and snoring in a child could probably improve a child’s life significantly. For exam-ple, if a child does not mouth breathe (day or night) nor snore, the mean number of symptoms present in such children consists of 2 symptoms. In those that both snore and mouth breathe the mean number of symptoms present is 9 symptoms. It would seem, there-fore, to successfully correct these two symptoms would probably have a great improvement in a child’s sleep problem. Such appli-ances commonly called the Habit Corrector and Healthy Start Kids are designed specifically to correct snor-ing and mouth breathing. CONCLUSION The results of this study suggest that 9 out of 10 children have at least one symptom of Sleep Disor-dered Breathing. Previous research found that SDB occurs in 1% to 3% of children from the ages of 5 to 13 years of age, however, the findings of this study provides evidence that SDB is much more common and effects children even as young as 2 years of age. 18 The implications of this study are essential in finding a way to improve the health of children today. Children begin to show symptoms of sleep disordered breathing as early as two years of age. It is essential that treatment to alleviate SDB in children begin as early as possible to ensure perma-nent dental changes in a growing child and the correction and promotion of proper oral habits in order to provide a long healthy life for these young children. This study supports the American Academy of Pediatric Dentistry’s (AAPD) push to have all children find a dental home by the age of one. 27 The find-ings of this study suggest that males are more susceptible to SDB and generally display more symptoms due to greater body mass. 28 This study provides evidence that mouth breathing maybe a more prominent indicator of SDB than that of snor-ing because it continues to be prominent throughout childhood unlike snoring where a large decrease is seen as children get older as seen in Fig. 8. As a result of this investigation the following conclusions can be made: ᕡ Mouth breathing and snoring are commonly associated with more SDB symptoms than the other symptoms studied. ᕢ The four most commonly occurring symptoms are: Mouth breathing at night, snoring, talks in sleep, and teeth grinding. ᕣ 90% of the sample had one or more symptoms commonly associated with SDB. ᕤ 60% of the sample had four or more symptoms. ᕥ Between 4 and 12 years of age, 92.6 % of symptoms did not self correct while 30% worsened with age. ᕦ The dentist is well positioned to be able to utilize appliances that can modify the most common symptoms. Editor’s Note: Click here for references. 28 Winter 2016 JAOS
Journal of the American Orthodontic Society Winter 2016: Page 28