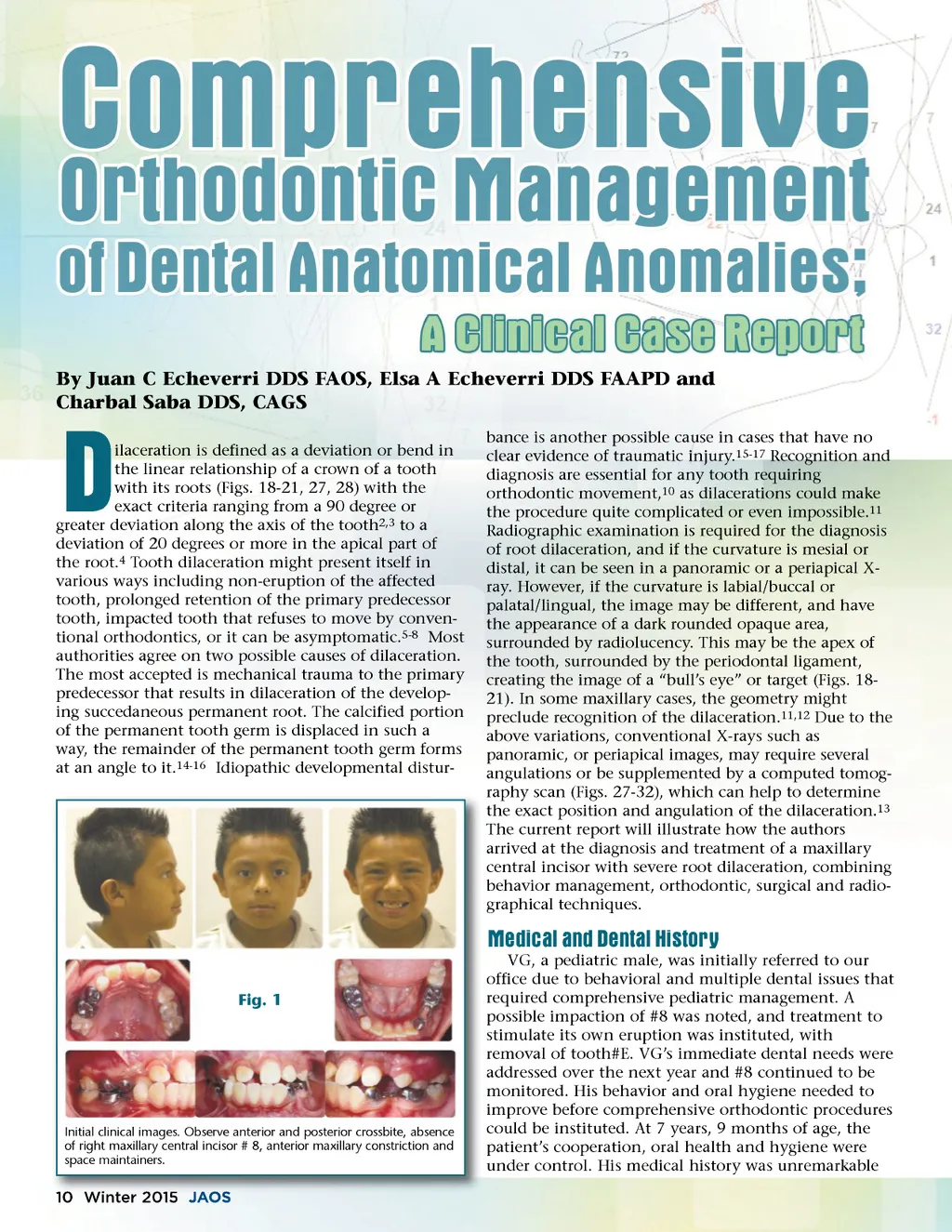
By Juan C Echeverri DDS FAOS, Elsa A Echeverri DDS FAAPD and Charbal Saba DDS, CAGS ilaceration is defined as a deviation or bend in the linear relationship of a crown of a tooth with its roots (Figs. 18-21, 27, 28) with the exact criteria ranging from a 90 degree or greater deviation along the axis of the tooth 2,3 to a deviation of 20 degrees or more in the apical part of the root. 4 Tooth dilaceration might present itself in various ways including non-eruption of the affected tooth, prolonged retention of the primary predecessor tooth, impacted tooth that refuses to move by conven-tional orthodontics, or it can be asymptomatic. 5-8 Most authorities agree on two possible causes of dilaceration. The most accepted is mechanical trauma to the primary predecessor that results in dilaceration of the develop-ing succedaneous permanent root. The calcified portion of the permanent tooth germ is displaced in such a way, the remainder of the permanent tooth germ forms at an angle to it. 14-16 Idiopathic developmental distur-D bance is another possible cause in cases that have no clear evidence of traumatic injury. 15-17 Recognition and diagnosis are essential for any tooth requiring orthodontic movement, 10 as dilacerations could make the procedure quite complicated or even impossible. 11 Radiographic examination is required for the diagnosis of root dilaceration, and if the curvature is mesial or distal, it can be seen in a panoramic or a periapical X-ray. However, if the curvature is labial/buccal or palatal/lingual, the image may be different, and have the appearance of a dark rounded opaque area, surrounded by radiolucency. This may be the apex of the tooth, surrounded by the periodontal ligament, creating the image of a “bull’s eye” or target (Figs. 18-21). In some maxillary cases, the geometry might preclude recognition of the dilaceration. 11,12 Due to the above variations, conventional X-rays such as panoramic, or periapical images, may require several angulations or be supplemented by a computed tomog-raphy scan (Figs. 27-32), which can help to determine the exact position and angulation of the dilaceration. 13 The current report will illustrate how the authors arrived at the diagnosis and treatment of a maxillary central incisor with severe root dilaceration, combining behavior management, orthodontic, surgical and radio-graphical techniques. Medical and Dental History Fig. 1 VG, a pediatric male, was initially referred to our office due to behavioral and multiple dental issues that required comprehensive pediatric management. A possible impaction of #8 was noted, and treatment to stimulate its own eruption was instituted, with removal of tooth#E. VG’s immediate dental needs were addressed over the next year and #8 continued to be monitored. His behavior and oral hygiene needed to improve before comprehensive orthodontic procedures could be instituted. At 7 years, 9 months of age, the patient’s cooperation, oral health and hygiene were under control. His medical history was unremarkable Initial clinical images. Observe anterior and posterior crossbite, absence of right maxillary central incisor # 8, anterior maxillary constriction and space maintainers. 10 Winter 2015 JAOS
Journal of the American Orthodontic Society Winter 2015: Page 10