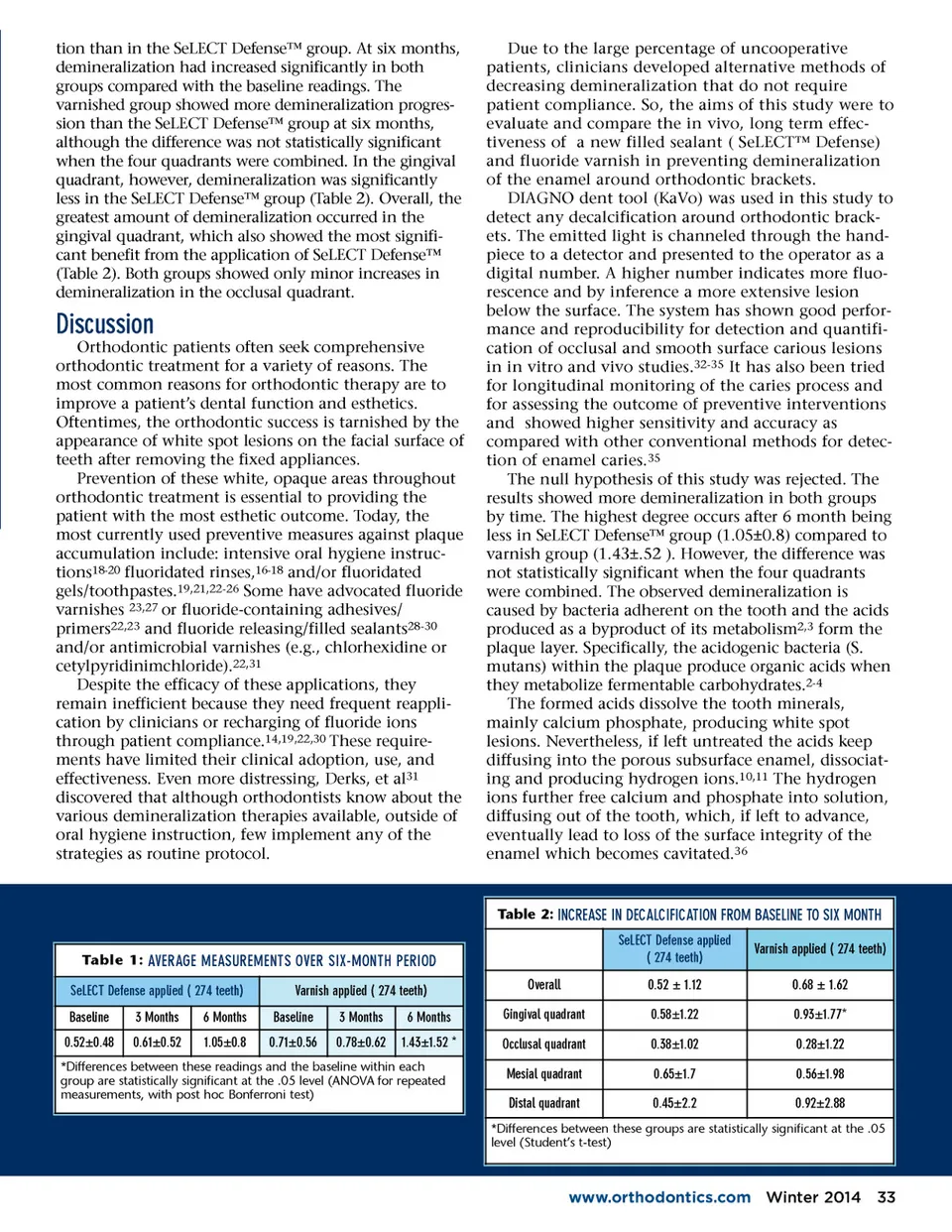
tion than in the SeLECT Defense™ group. At six months, demineralization had increased significantly in both groups compared with the baseline readings. The varnished group showed more demineralization progres-sion than the SeLECT Defense™ group at six months, although the difference was not statistically significant when the four quadrants were combined. In the gingival quadrant, however, demineralization was significantly less in the SeLECT Defense™ group (Table 2). Overall, the greatest amount of demineralization occurred in the gingival quadrant, which also showed the most signifi-cant benefit from the application of SeLECT Defense™ (Table 2). Both groups showed only minor increases in demineralization in the occlusal quadrant. Discussion Orthodontic patients often seek comprehensive orthodontic treatment for a variety of reasons. The most common reasons for orthodontic therapy are to improve a patient’s dental function and esthetics. Oftentimes, the orthodontic success is tarnished by the appearance of white spot lesions on the facial surface of teeth after removing the fixed appliances. Prevention of these white, opaque areas throughout orthodontic treatment is essential to providing the patient with the most esthetic outcome. Today, the most currently used preventive measures against plaque accumulation include: intensive oral hygiene instruc-tions 18-20 fluoridated rinses, 16-18 and/or fluoridated gels/toothpastes. 19,21,22-26 Some have advocated fluoride varnishes 23,27 or fluoride-containing adhesives/ primers 22,23 and fluoride releasing/filled sealants 28-30 and/or antimicrobial varnishes (e.g., chlorhexidine or cetylpyridinimchloride). 22,31 Despite the efficacy of these applications, they remain inefficient because they need frequent reappli-cation by clinicians or recharging of fluoride ions through patient compliance. 14,19,22,30 These require-ments have limited their clinical adoption, use, and effectiveness. Even more distressing, Derks, et al 31 discovered that although orthodontists know about the various demineralization therapies available, outside of oral hygiene instruction, few implement any of the strategies as routine protocol. Due to the large percentage of uncooperative patients, clinicians developed alternative methods of decreasing demineralization that do not require patient compliance. So, the aims of this study were to evaluate and compare the in vivo, long term effec-tiveness of a new filled sealant ( SeLECT™ Defense) and fluoride varnish in preventing demineralization of the enamel around orthodontic brackets. DIAGNO dent tool (KaVo) was used in this study to detect any decalcification around orthodontic brack-ets. The emitted light is channeled through the hand-piece to a detector and presented to the operator as a digital number. A higher number indicates more fluo-rescence and by inference a more extensive lesion below the surface. The system has shown good perfor-mance and reproducibility for detection and quantifi-cation of occlusal and smooth surface carious lesions in in vitro and vivo studies. 32-35 It has also been tried for longitudinal monitoring of the caries process and for assessing the outcome of preventive interventions and showed higher sensitivity and accuracy as compared with other conventional methods for detec-tion of enamel caries. 35 The null hypothesis of this study was rejected. The results showed more demineralization in both groups by time. The highest degree occurs after 6 month being less in SeLECT Defense™ group (1.05±0.8) compared to varnish group (1.43±.52 ). However, the difference was not statistically significant when the four quadrants were combined. The observed demineralization is caused by bacteria adherent on the tooth and the acids produced as a byproduct of its metabolism 2,3 form the plaque layer. Specifically, the acidogenic bacteria (S. mutans) within the plaque produce organic acids when they metabolize fermentable carbohydrates. 2-4 The formed acids dissolve the tooth minerals, mainly calcium phosphate, producing white spot lesions. Nevertheless, if left untreated the acids keep diffusing into the porous subsurface enamel, dissociat-ing and producing hydrogen ions. 10,11 The hydrogen ions further free calcium and phosphate into solution, diffusing out of the tooth, which, if left to advance, eventually lead to loss of the surface integrity of the enamel which becomes cavitated. 36 Table 2: INCREASE IN DECALCIFICATION FROM BASELINE TO SIX MONTH Table 1: AVERAGE MEASUREMENTS OVER SIX-MONTH PERIOD SeLECT Defense applied ( 274 teeth) Baseline 0.52±0.48 3 Months 0.61±0.52 6 Months 1.05±0.8 Varnish applied ( 274 teeth) Baseline 0.71±0.56 3 Months 0.78±0.62 6 Months 1.43±1.52 * Overall Gingival quadrant Occlusal quadrant Mesial quadrant Distal quadrant SeLECT Defense applied ( 274 teeth) 0.52 ± 1.12 0.58±1.22 0.38±1.02 0.65±1.7 0.45±2.2 Varnish applied ( 274 teeth) 0.68 ± 1.62 0.93±1.77* 0.28±1.22 0.56±1.98 0.92±2.88 *Differences between these readings and the baseline within each group are statistically significant at the .05 level (ANOVA for repeated measurements, with post hoc Bonferroni test) *Differences between these groups are statistically significant at the .05 level (Student’s t-test) www.orthodontics.com Winter 2014 33
Journal of the American Orthodontic Society Winter 2014: Page 33