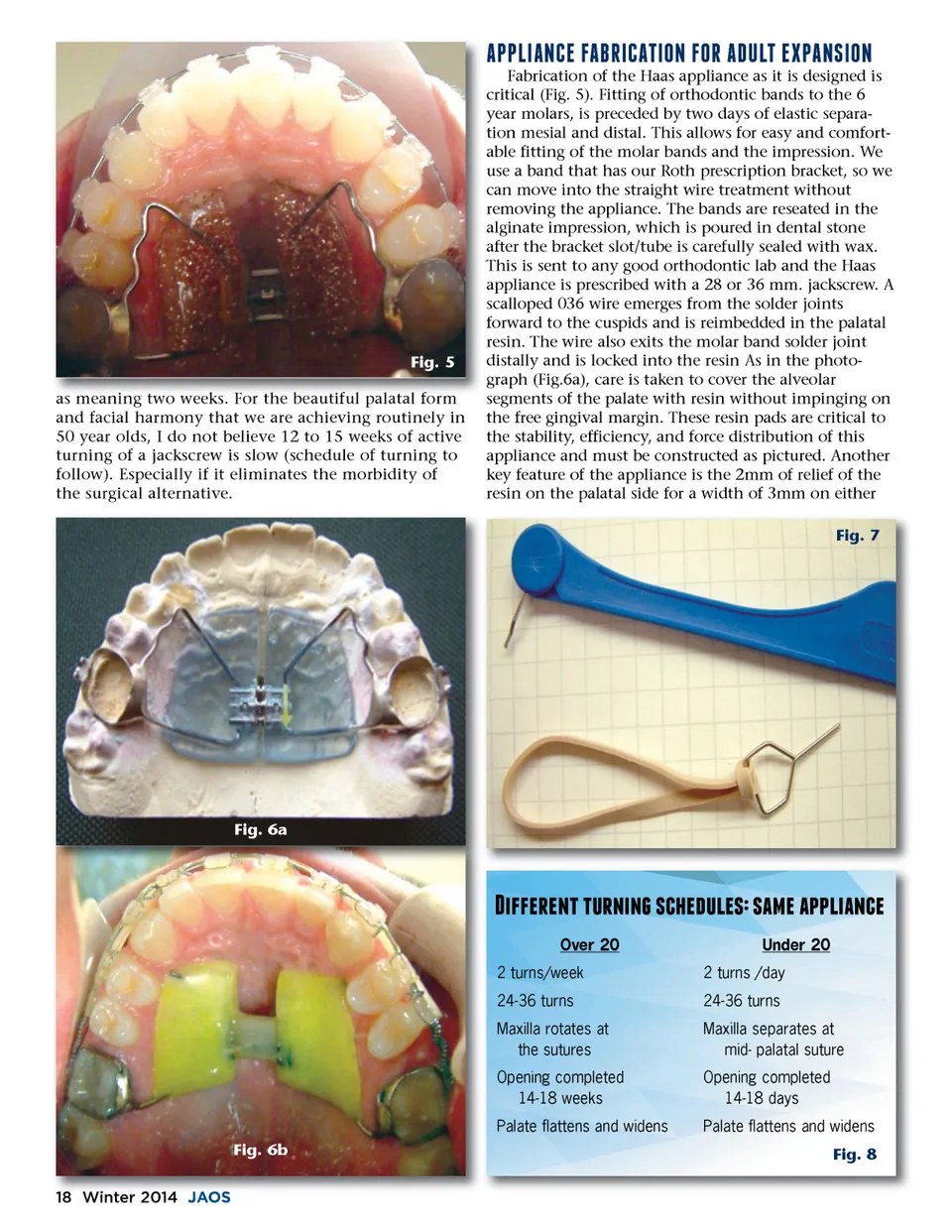
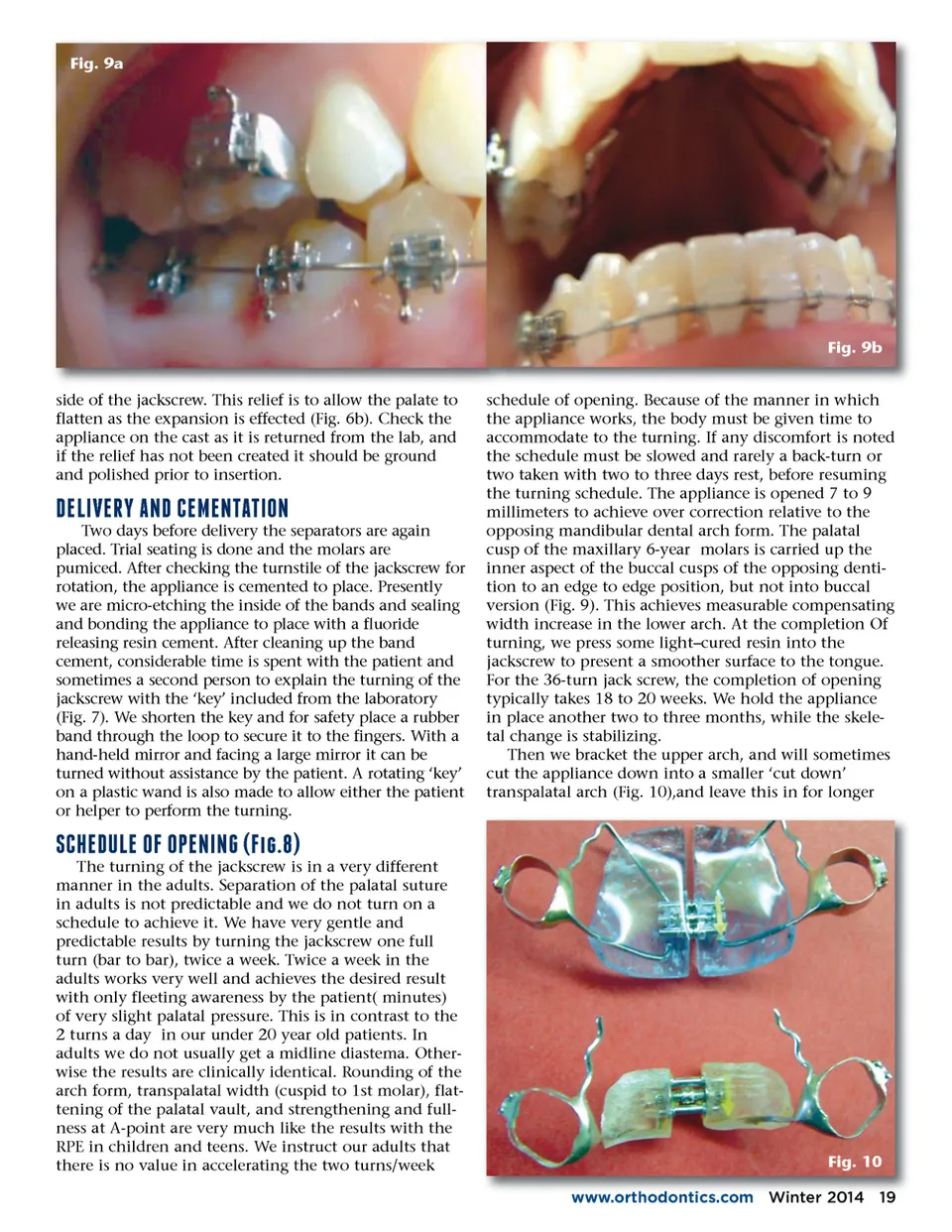
Fig. 9a Fig. 9b side of the jackscrew. This relief is to allow the palate to flatten as the expansion is effected (Fig. 6b). Check the appliance on the cast as it is returned from the lab, and if the relief has not been created it should be ground and polished prior to insertion. schedule of opening. Because of the manner in which the appliance works, the body must be given time to accommodate to the turning. If any discomfort is noted the schedule must be slowed and rarely a back-turn or two taken with two to three days rest, before resuming the turning schedule. The appliance is opened 7 to 9 millimeters to achieve over correction relative to the opposing mandibular dental arch form. The palatal cusp of the maxillary 6-year molars is carried up the inner aspect of the buccal cusps of the opposing denti-tion to an edge to edge position, but not into buccal version (Fig. 9). This achieves measurable compensating width increase in the lower arch. At the completion Of turning, we press some light–cured resin into the jackscrew to present a smoother surface to the tongue. For the 36-turn jack screw, the completion of opening typically takes 18 to 20 weeks. We hold the appliance in place another two to three months, while the skele-tal change is stabilizing. Then we bracket the upper arch, and will sometimes cut the appliance down into a smaller ‘cut down’ transpalatal arch (Fig. 10),and leave this in for longer f;0e;-�b;0b;7+.f;7&0�e;0.'+'-".7 Two days before delivery the separators are again placed. Trial seating is done and the molars are pumiced. After checking the turnstile of the jackscrew for rotation, the appliance is cemented to place. Presently we are micro-etching the inside of the bands and sealing and bonding the appliance to place with a fluoride releasing resin cement. After cleaning up the band cement, considerable time is spent with the patient and sometimes a second person to explain the turning of the jackscrew with the ‘key’ included from the laboratory (Fig. 7). We shorten the key and for safety place a rubber band through the loop to secure it to the fingers. With a hand-held mirror and facing a large mirror it can be turned without assistance by the patient. A rotating ‘key’ on a plastic wand is also made to allow either the patient or helper to perform the turning. !&0f;e;07"c;7"a;0.-.7c;4d; 7 The turning of the jackscrew is in a very different manner in the adults. Separation of the palatal suture in adults is not predictable and we do not turn on a schedule to achieve it. We have very gentle and predictable results by turning the jackscrew one full turn (bar to bar), twice a week. Twice a week in the adults works very well and achieves the desired result with only fleeting awareness by the patient( minutes) of very slight palatal pressure. This is in contrast to the 2 turns a day in our under 20 year old patients. In adults we do not usually get a midline diastema. Other-wise the results are clinically identical. Rounding of the arch form, transpalatal width (cuspid to 1st molar), flat-tening of the palatal vault, and strengthening and full-ness at A-point are very much like the results with the RPE in children and teens. We instruct our adults that there is no value in accelerating the two turns/week Fig. 10 www.orthodontics.com www orthodontics com Winter 2014 19
Journal of the American Orthodontic Society Winter 2014: Page 19