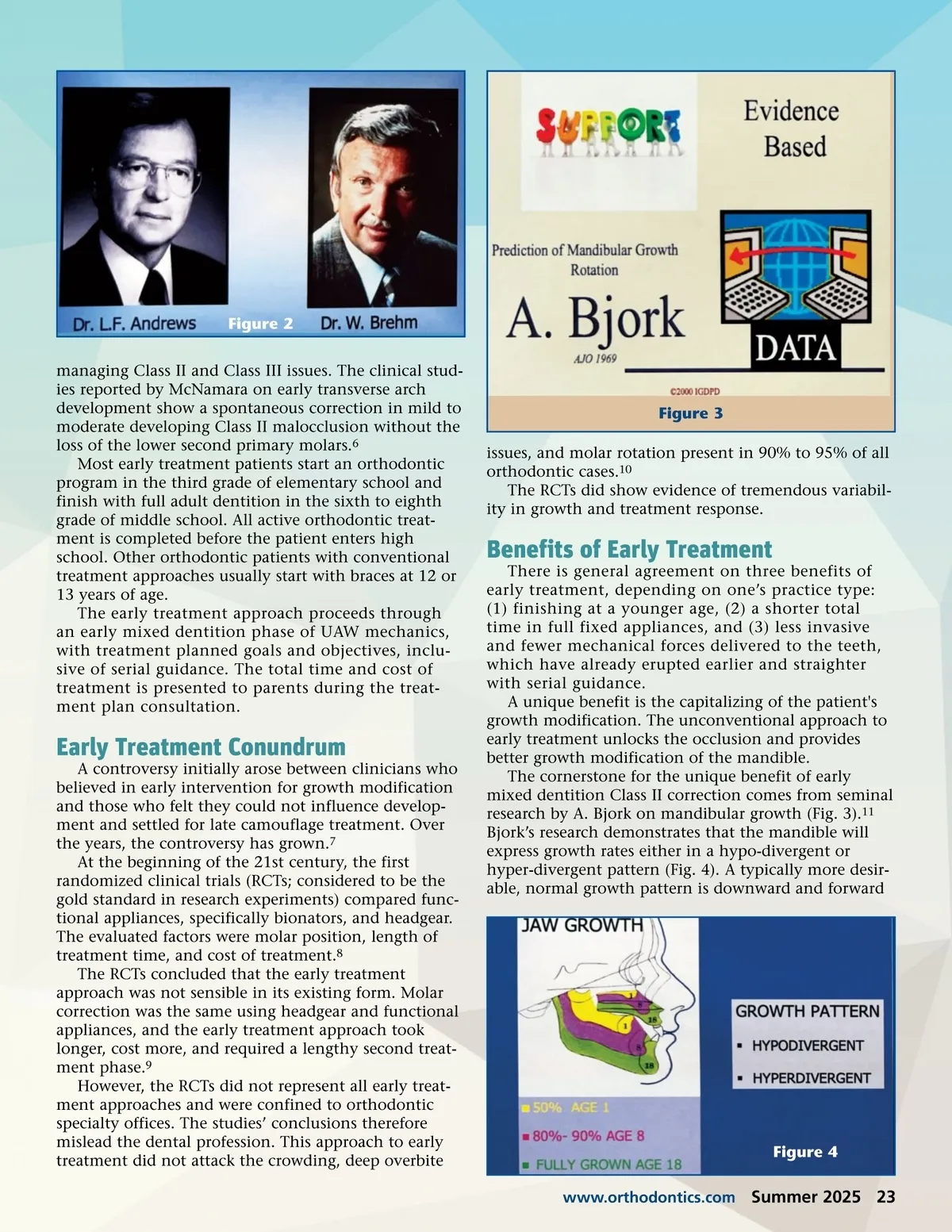
Figure 2 managing Class II and Class III issues. The clinical stud-ies reported by McNamara on early transverse arch development show a spontaneous correction in mild to moderate developing Class II malocclusion without the loss of the lower second primary molars. 6 Most early treatment patients start an orthodontic program in the third grade of elementary school and finish with full adult dentition in the sixth to eighth grade of middle school. All active orthodontic treat-ment is completed before the patient enters high school. Other orthodontic patients with conventional treatment approaches usually start with braces at 12 or 13 years of age. The early treatment approach proceeds through an early mixed dentition phase of UAW mechanics, with treatment planned goals and objectives, inclu-sive of serial guidance. The total time and cost of treatment is presented to parents during the treat-ment plan consultation. Figure 3 issues, and molar rotation present in 90% to 95% of all orthodontic cases. 10 The RCTs did show evidence of tremendous variabil-ity in growth and treatment response. Benefits of Early Treatment There is general agreement on three benefits of early treatment, depending on one’s practice type: (1) finishing at a younger age, (2) a shorter total time in full fixed appliances, and (3) less invasive and fewer mechanical forces delivered to the teeth, which have already erupted earlier and straighter with serial guidance. A unique benefit is the capitalizing of the patient's growth modification. The unconventional approach to early treatment unlocks the occlusion and provides better growth modification of the mandible. The cornerstone for the unique benefit of early mixed dentition Class II correction comes from seminal research by A. Bjork on mandibular growth (Fig. 3). 11 Bjork’s research demonstrates that the mandible will express growth rates either in a hypo-divergent or hyper-divergent pattern (Fig. 4). A typically more desir-able, normal growth pattern is downward and forward Early Treatment Conundrum A controversy initially arose between clinicians who believed in early intervention for growth modification and those who felt they could not influence develop-ment and settled for late camouflage treatment. Over the years, the controversy has grown. 7 At the beginning of the 21st century, the first randomized clinical trials (RCTs; considered to be the gold standard in research experiments) compared func-tional appliances, specifically bionators, and headgear. The evaluated factors were molar position, length of treatment time, and cost of treatment. 8 The RCTs concluded that the early treatment approach was not sensible in its existing form. Molar correction was the same using headgear and functional appliances, and the early treatment approach took longer, cost more, and required a lengthy second treat-ment phase. 9 However, the RCTs did not represent all early treat-ment approaches and were confined to orthodontic specialty offices. The studies’ conclusions therefore mislead the dental profession. This approach to early treatment did not attack the crowding, deep overbite Figure 4 www.orthodontics.com Summer 2025 23
Journal of the American Orthodontic Society Summer 2025: Page 23