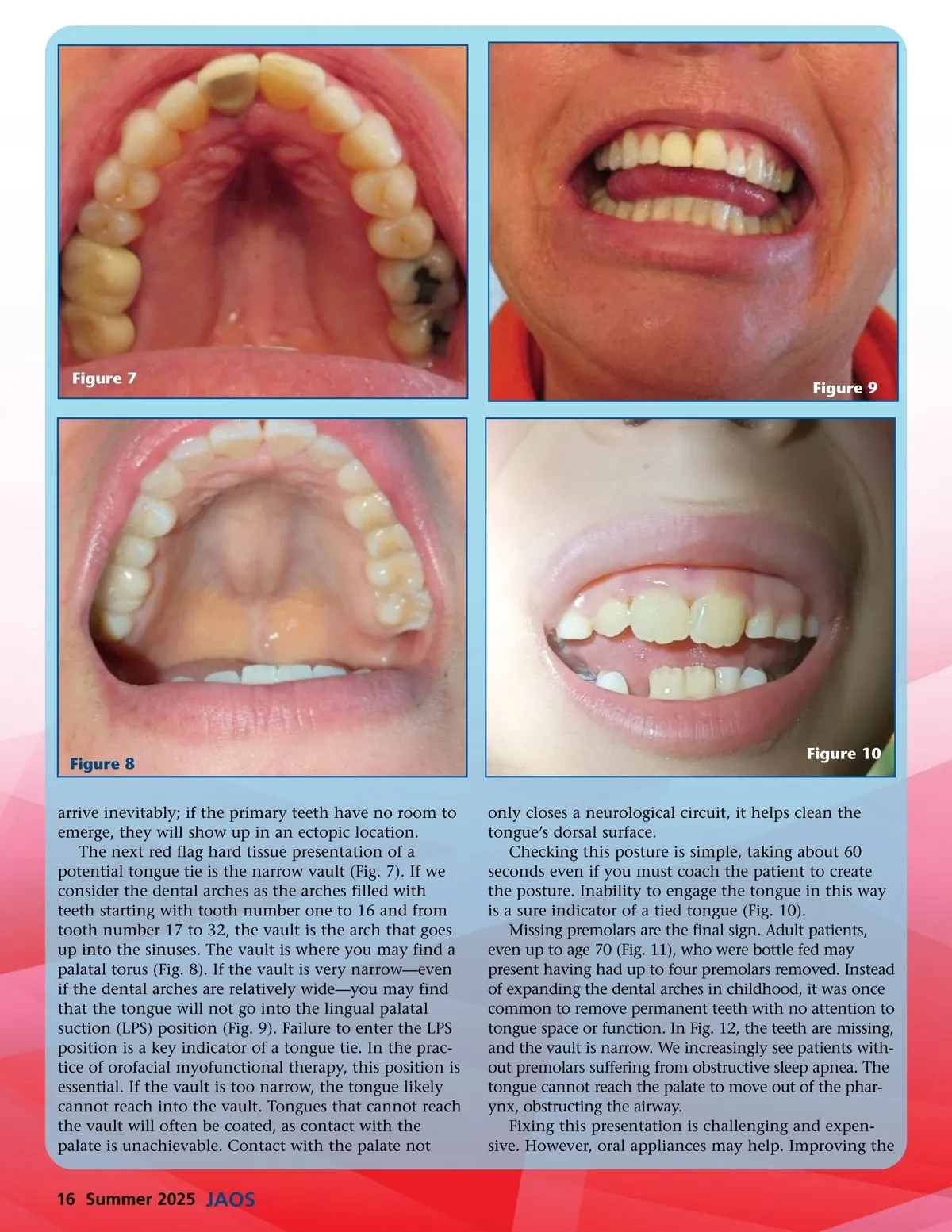
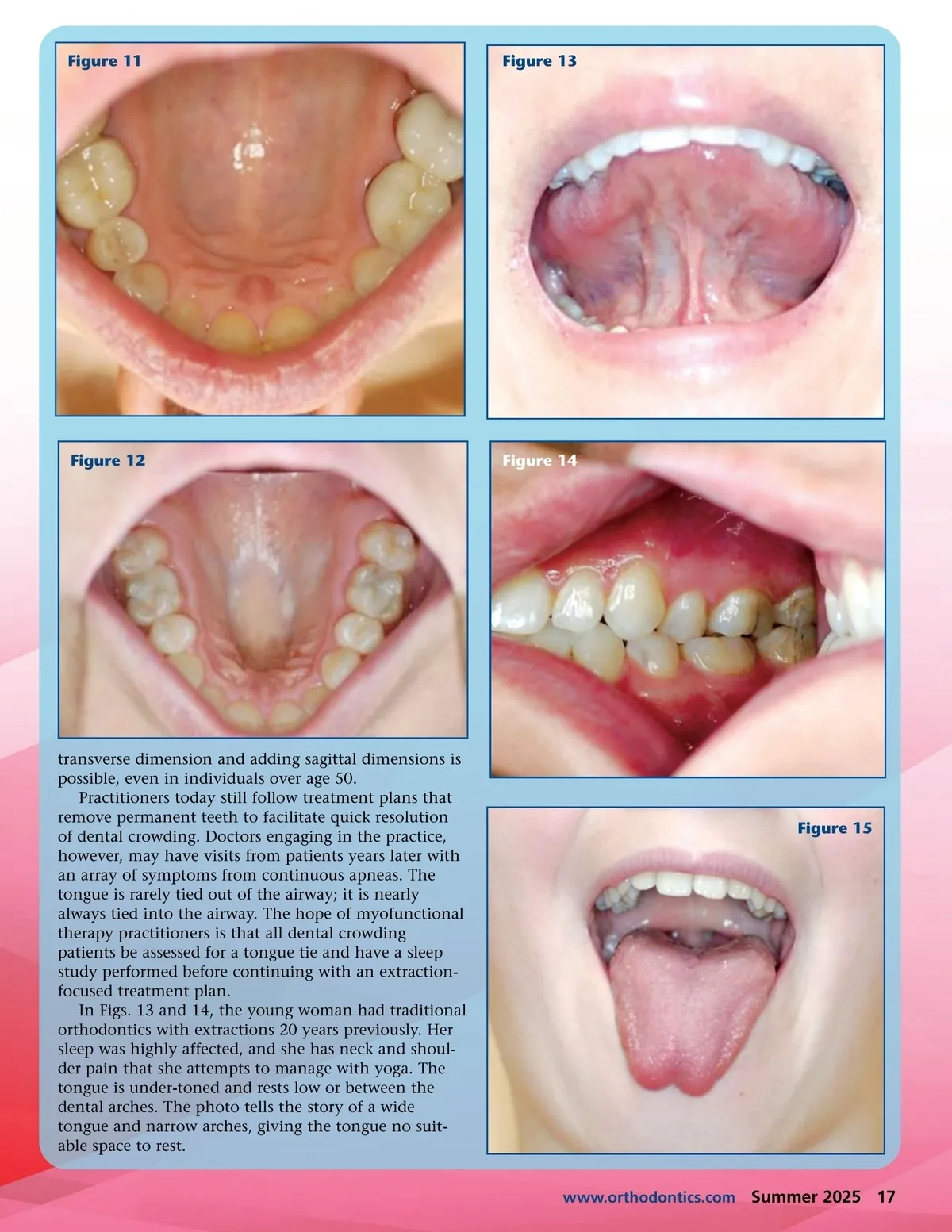
Figure 7 Figure 9 Figure 8 arrive inevitably; if the primary teeth have no room to emerge, they will show up in an ectopic location. The next red flag hard tissue presentation of a potential tongue tie is the narrow vault (Fig. 7). If we consider the dental arches as the arches filled with teeth starting with tooth number one to 16 and from tooth number 17 to 32, the vault is the arch that goes up into the sinuses. The vault is where you may find a palatal torus (Fig. 8). If the vault is very narrow—even if the dental arches are relatively wide—you may find that the tongue will not go into the lingual palatal suction (LPS) position (Fig. 9). Failure to enter the LPS position is a key indicator of a tongue tie. In the prac-tice of orofacial myofunctional therapy, this position is essential. If the vault is too narrow, the tongue likely cannot reach into the vault. Tongues that cannot reach the vault will often be coated, as contact with the palate is unachievable. Contact with the palate not Figure 10 only closes a neurological circuit, it helps clean the tongue’s dorsal surface. Checking this posture is simple, taking about 60 seconds even if you must coach the patient to create the posture. Inability to engage the tongue in this way is a sure indicator of a tied tongue (Fig. 10). Missing premolars are the final sign. Adult patients, even up to age 70 (Fig. 11), who were bottle fed may present having had up to four premolars removed. Instead of expanding the dental arches in childhood, it was once common to remove permanent teeth with no attention to tongue space or function. In Fig. 12, the teeth are missing, and the vault is narrow. We increasingly see patients with-out premolars suffering from obstructive sleep apnea. The tongue cannot reach the palate to move out of the phar-ynx, obstructing the airway. Fixing this presentation is challenging and expen-sive. However, oral appliances may help. Improving the 16 Summer 2025 JAOS
Journal of the American Orthodontic Society Summer 2025: Page 16