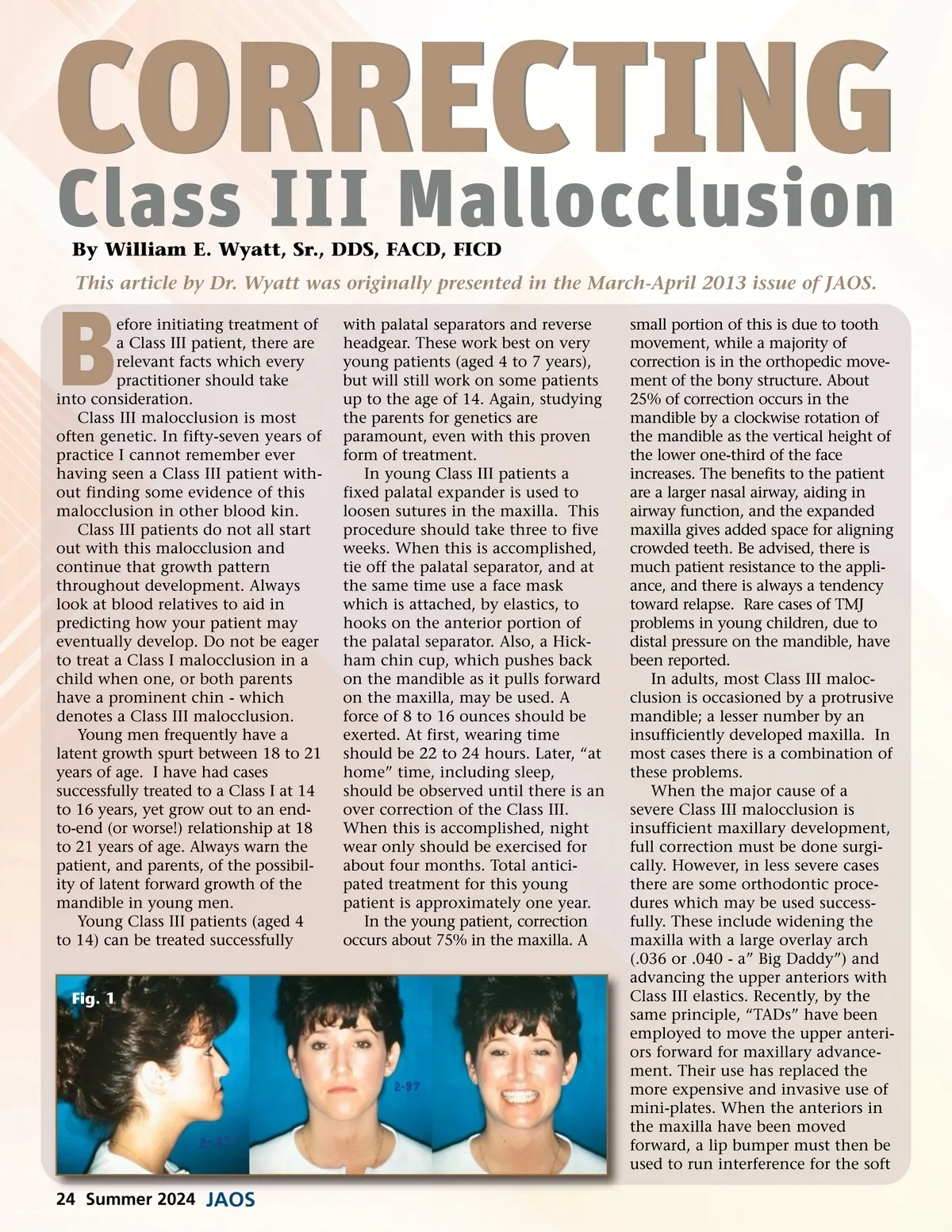
CORRECTING Class III Mallocclusion By William E. Wyatt, Sr., DDS, FACD, FICD This article by Dr. Wyatt was originally presented in the March-April 2013 issue of JAOS. B efore initiating treatment of a Class III patient, there are relevant facts which every practitioner should take into consideration. Class III malocclusion is most often genetic. In fifty-seven years of practice I cannot remember ever having seen a Class III patient with-out finding some evidence of this malocclusion in other blood kin. Class III patients do not all start out with this malocclusion and continue that growth pattern throughout development. Always look at blood relatives to aid in predicting how your patient may eventually develop. Do not be eager to treat a Class I malocclusion in a child when one, or both parents have a prominent chin -which denotes a Class III malocclusion. Young men frequently have a latent growth spurt between 18 to 21 years of age. I have had cases successfully treated to a Class I at 14 to 16 years, yet grow out to an end-to-end (or worse!) relationship at 18 to 21 years of age. Always warn the patient, and parents, of the possibil-ity of latent forward growth of the mandible in young men. Young Class III patients (aged 4 to 14) can be treated successfully with palatal separators and reverse headgear. These work best on very young patients (aged 4 to 7 years), but will still work on some patients up to the age of 14. Again, studying the parents for genetics are paramount, even with this proven form of treatment. In young Class III patients a fixed palatal expander is used to loosen sutures in the maxilla. This procedure should take three to five weeks. When this is accomplished, tie off the palatal separator, and at the same time use a face mask which is attached, by elastics, to hooks on the anterior portion of the palatal separator. Also, a Hick-ham chin cup, which pushes back on the mandible as it pulls forward on the maxilla, may be used. A force of 8 to 16 ounces should be exerted. At first, wearing time should be 22 to 24 hours. Later, “at home” time, including sleep, should be observed until there is an over correction of the Class III. When this is accomplished, night wear only should be exercised for about four months. Total antici-pated treatment for this young patient is approximately one year. In the young patient, correction occurs about 75% in the maxilla. A Fig. 1 small portion of this is due to tooth movement, while a majority of correction is in the orthopedic move-ment of the bony structure. About 25% of correction occurs in the mandible by a clockwise rotation of the mandible as the vertical height of the lower one-third of the face increases. The benefits to the patient are a larger nasal airway, aiding in airway function, and the expanded maxilla gives added space for aligning crowded teeth. Be advised, there is much patient resistance to the appli-ance, and there is always a tendency toward relapse. Rare cases of TMJ problems in young children, due to distal pressure on the mandible, have been reported. In adults, most Class III maloc-clusion is occasioned by a protrusive mandible; a lesser number by an insufficiently developed maxilla. In most cases there is a combination of these problems. When the major cause of a severe Class III malocclusion is insufficient maxillary development, full correction must be done surgi-cally. However, in less severe cases there are some orthodontic proce-dures which may be used success-fully. These include widening the maxilla with a large overlay arch (.036 or .040 -a” Big Daddy”) and advancing the upper anteriors with Class III elastics. Recently, by the same principle, “TADs” have been employed to move the upper anteri-ors forward for maxillary advance-ment. Their use has replaced the more expensive and invasive use of mini-plates. When the anteriors in the maxilla have been moved forward, a lip bumper must then be used to run interference for the soft 24 Summer 2024 JAOS
Journal of the American Orthodontic Society Summer 2024: Page 24