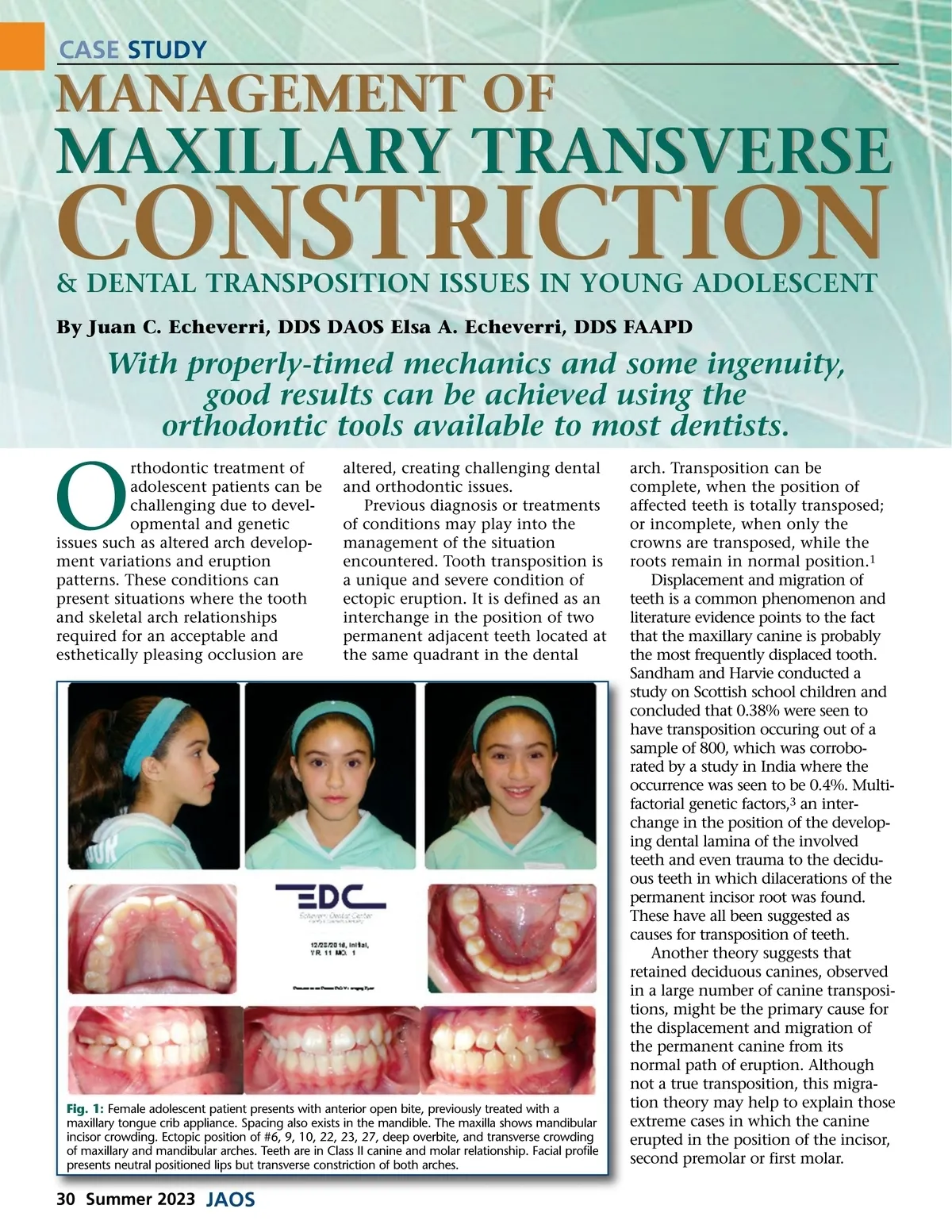
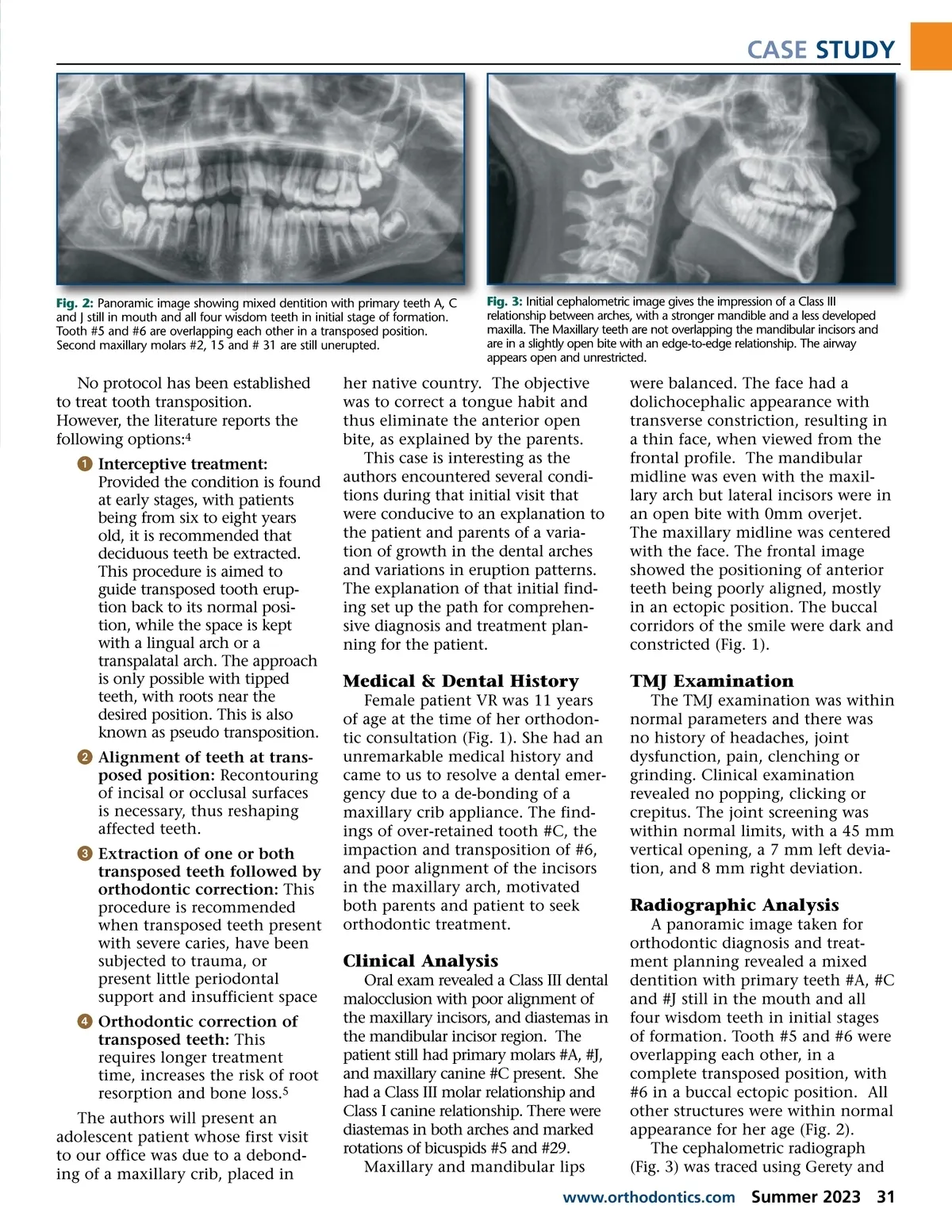
CASE STUDY Fig. 2: Panoramic image showing mixed dentition with primary teeth A, C and J still in mouth and all four wisdom teeth in initial stage of formation. Tooth #5 and #6 are overlapping each other in a transposed position. Second maxillary molars #2, 15 and # 31 are still unerupted. Fig. 3: Initial cephalometric image gives the impression of a Class III relationship between arches, with a stronger mandible and a less developed maxilla. The Maxillary teeth are not overlapping the mandibular incisors and are in a slightly open bite with an edge-to-edge relationship. The airway appears open and unrestricted. No protocol has been established to treat tooth transposition. However, the literature reports the following options: 4 ᕡ Interceptive treatment: Provided the condition is found at early stages, with patients being from six to eight years old, it is recommended that deciduous teeth be extracted. This procedure is aimed to guide transposed tooth erup-tion back to its normal posi-tion, while the space is kept with a lingual arch or a transpalatal arch. The approach is only possible with tipped teeth, with roots near the desired position. This is also known as pseudo transposition. ᕢ Alignment of teeth at trans-posed position: Recontouring of incisal or occlusal surfaces is necessary, thus reshaping affected teeth. ᕣ Extraction of one or both transposed teeth followed by orthodontic correction: This procedure is recommended when transposed teeth present with severe caries, have been subjected to trauma, or present little periodontal support and insufficient space ᕤ Orthodontic correction of transposed teeth: This requires longer treatment time, increases the risk of root resorption and bone loss. 5 The authors will present an adolescent patient whose first visit to our office was due to a debond-ing of a maxillary crib, placed in her native country. The objective was to correct a tongue habit and thus eliminate the anterior open bite, as explained by the parents. This case is interesting as the authors encountered several condi-tions during that initial visit that were conducive to an explanation to the patient and parents of a varia-tion of growth in the dental arches and variations in eruption patterns. The explanation of that initial find-ing set up the path for comprehen-sive diagnosis and treatment plan-ning for the patient. were balanced. The face had a dolichocephalic appearance with transverse constriction, resulting in a thin face, when viewed from the frontal profile. The mandibular midline was even with the maxil-lary arch but lateral incisors were in an open bite with 0mm overjet. The maxillary midline was centered with the face. The frontal image showed the positioning of anterior teeth being poorly aligned, mostly in an ectopic position. The buccal corridors of the smile were dark and constricted (Fig. 1). Medical & Dental History Female patient VR was 11 years of age at the time of her orthodon-tic consultation (Fig. 1). She had an unremarkable medical history and came to us to resolve a dental emer-gency due to a de-bonding of a maxillary crib appliance. The find-ings of over-retained tooth #C, the impaction and transposition of #6, and poor alignment of the incisors in the maxillary arch, motivated both parents and patient to seek orthodontic treatment. TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunction, pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a 45 mm vertical opening, a 7 mm left devia-tion, and 8 mm right deviation. Radiographic Analysis A panoramic image taken for orthodontic diagnosis and treat-ment planning revealed a mixed dentition with primary teeth #A, #C and #J still in the mouth and all four wisdom teeth in initial stages of formation. Tooth #5 and #6 were overlapping each other, in a complete transposed position, with #6 in a buccal ectopic position. All other structures were within normal appearance for her age (Fig. 2). The cephalometric radiograph (Fig. 3) was traced using Gerety and Clinical Analysis Oral exam revealed a Class III dental malocclusion with poor alignment of the maxillary incisors, and diastemas in the mandibular incisor region. The patient still had primary molars #A, #J, and maxillary canine #C present. She had a Class III molar relationship and Class I canine relationship. There were diastemas in both arches and marked rotations of bicuspids #5 and #29. Maxillary and mandibular lips www.orthodontics.com Summer 2023 31
Journal of the American Orthodontic Society Summer 2023: Page 31