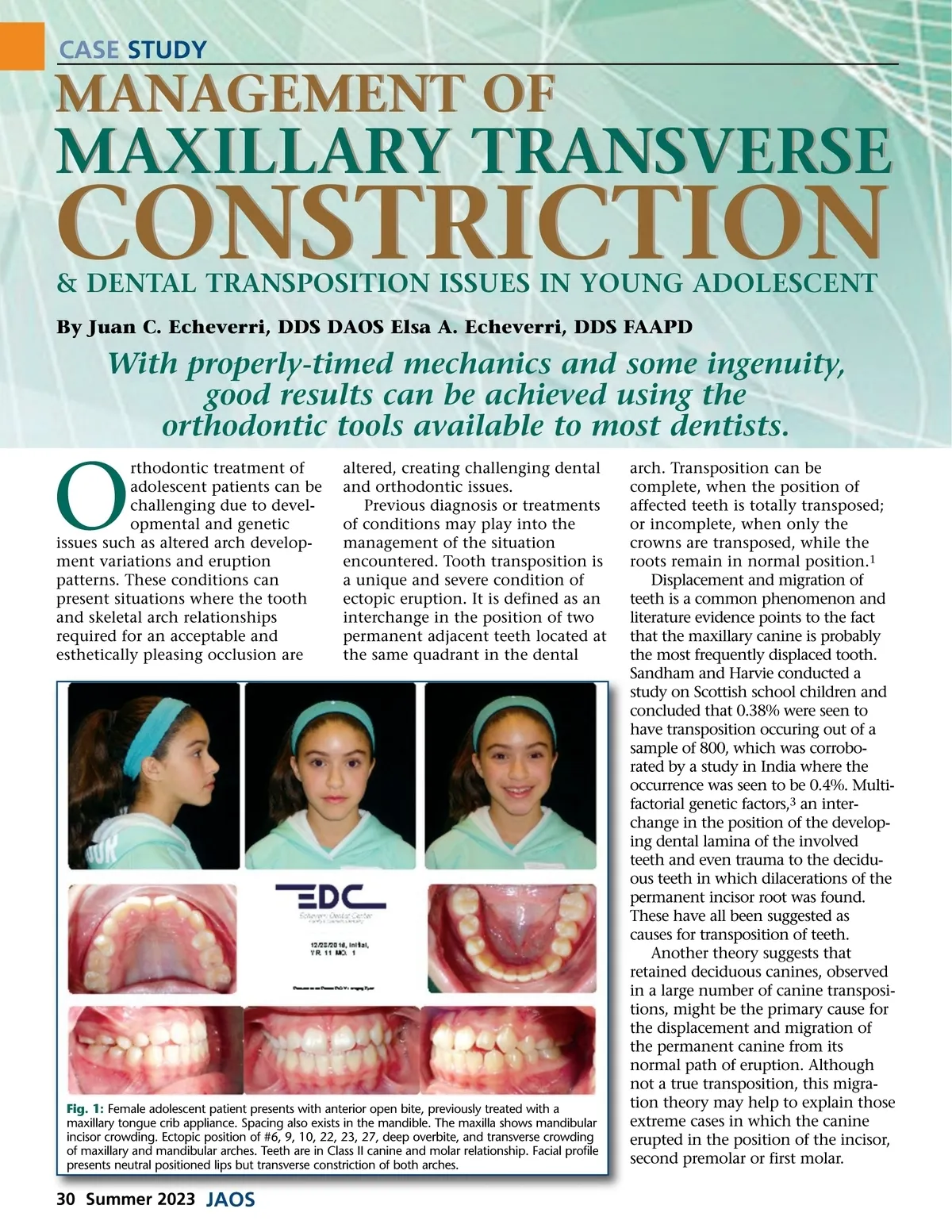
CASE STUDY MANAGEMENT OF MAXILLARY TRANSVERSE CONSTRICTION & DENTAL TRANSPOSITION ISSUES IN YOUNG ADOLESCENT By Juan C. Echeverri, DDS DAOS Elsa A. Echeverri, DDS FAAPD With properly-timed mechanics and some ingenuity, good results can be achieved using the orthodontic tools available to most dentists. O rthodontic treatment of adolescent patients can be challenging due to devel-opmental and genetic issues such as altered arch develop-ment variations and eruption patterns. These conditions can present situations where the tooth and skeletal arch relationships required for an acceptable and esthetically pleasing occlusion are altered, creating challenging dental and orthodontic issues. Previous diagnosis or treatments of conditions may play into the management of the situation encountered. Tooth transposition is a unique and severe condition of ectopic eruption. It is defined as an interchange in the position of two permanent adjacent teeth located at the same quadrant in the dental Fig. 1: Female adolescent patient presents with anterior open bite, previously treated with a maxillary tongue crib appliance. Spacing also exists in the mandible. The maxilla shows mandibular incisor crowding. Ectopic position of #6, 9, 10, 22, 23, 27, deep overbite, and transverse crowding of maxillary and mandibular arches. Teeth are in Class II canine and molar relationship. Facial profile presents neutral positioned lips but transverse constriction of both arches. arch. Transposition can be complete, when the position of affected teeth is totally transposed; or incomplete, when only the crowns are transposed, while the roots remain in normal position. 1 Displacement and migration of teeth is a common phenomenon and literature evidence points to the fact that the maxillary canine is probably the most frequently displaced tooth. Sandham and Harvie conducted a study on Scottish school children and concluded that 0.38% were seen to have transposition occuring out of a sample of 800, which was corrobo-rated by a study in India where the occurrence was seen to be 0.4%. Multi-factorial genetic factors, 3 an inter-change in the position of the develop-ing dental lamina of the involved teeth and even trauma to the decidu-ous teeth in which dilacerations of the permanent incisor root was found. These have all been suggested as causes for transposition of teeth. Another theory suggests that retained deciduous canines, observed in a large number of canine transposi-tions, might be the primary cause for the displacement and migration of the permanent canine from its normal path of eruption. Although not a true transposition, this migra-tion theory may help to explain those extreme cases in which the canine erupted in the position of the incisor, second premolar or first molar. 30 Summer 2023 JAOS
Journal of the American Orthodontic Society Summer 2023: Page 30