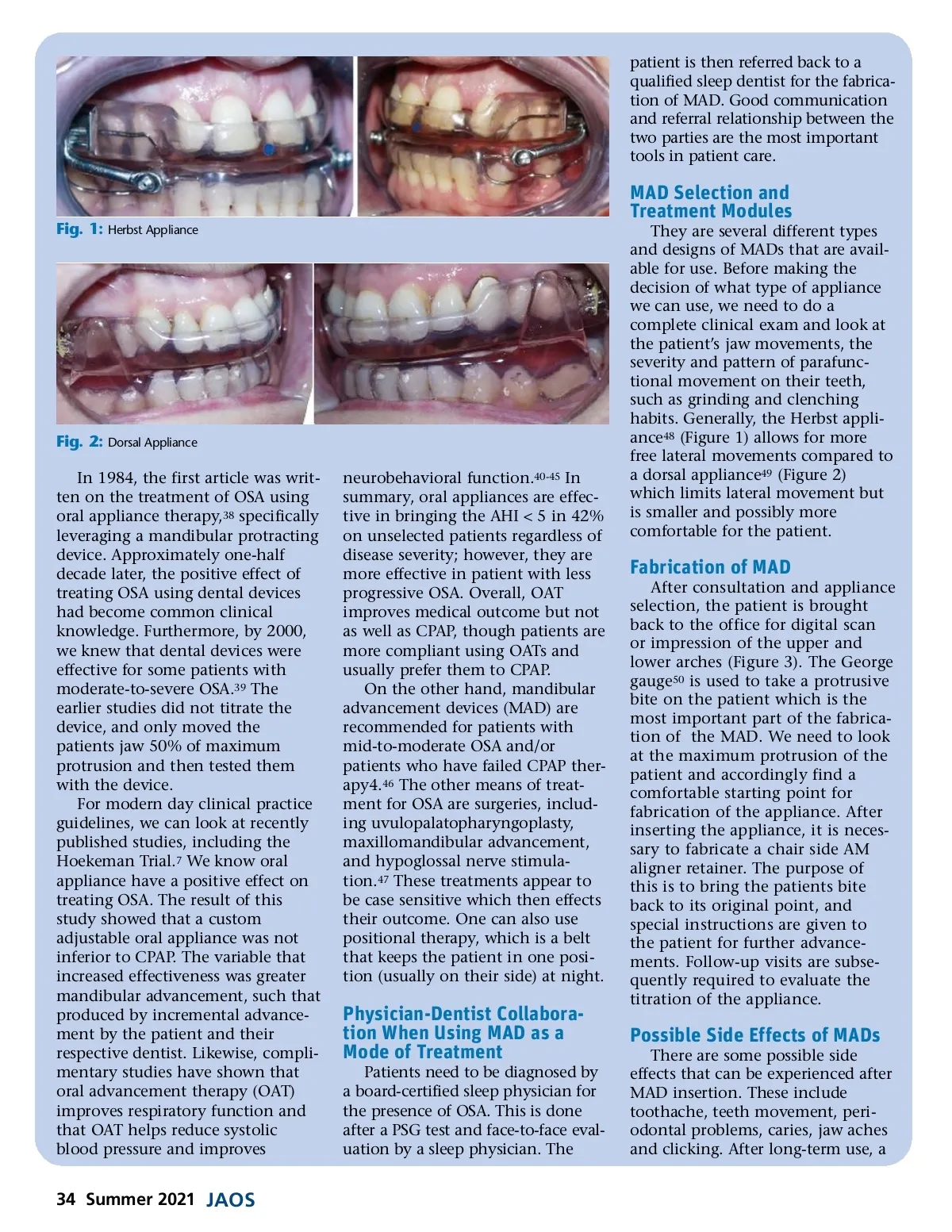
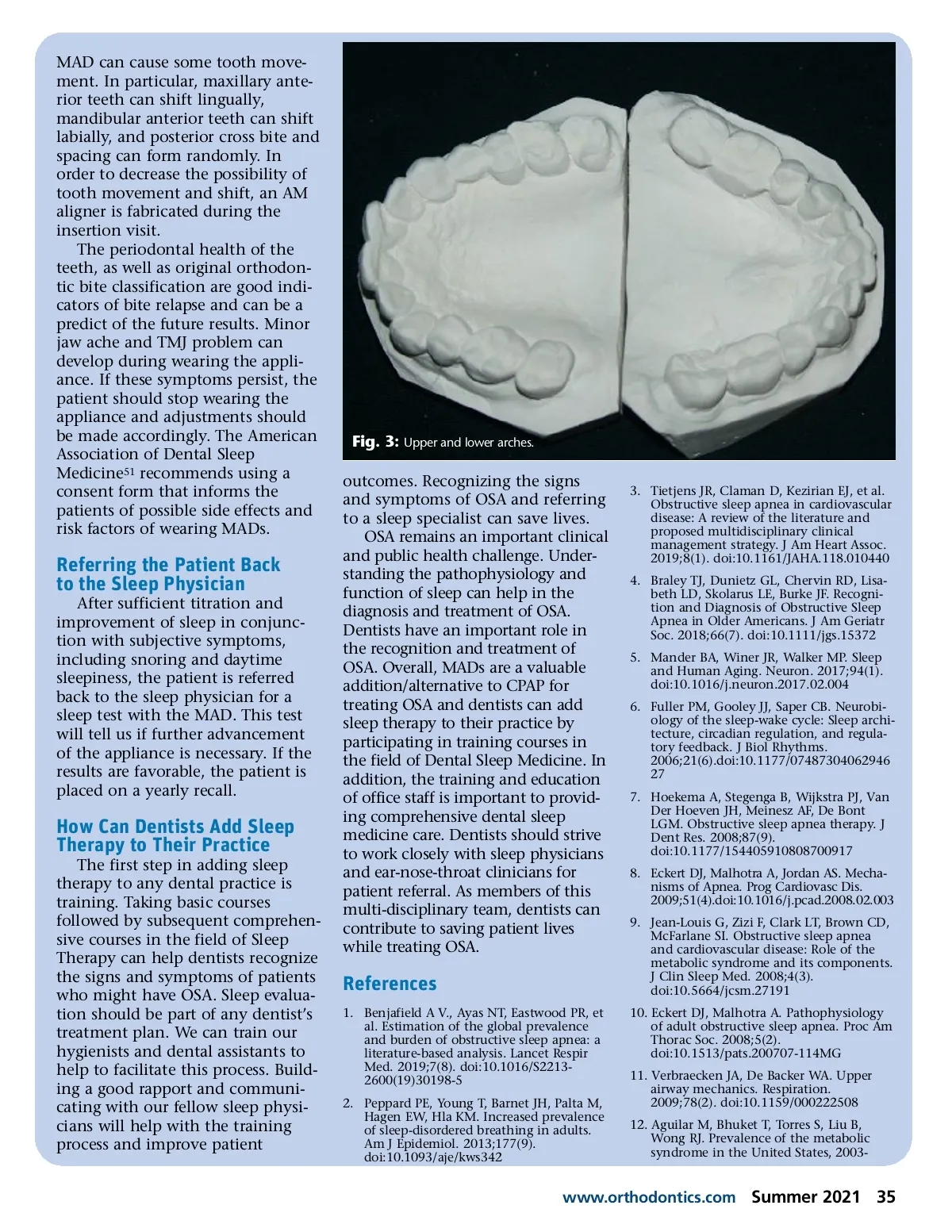
MAD can cause some tooth move-ment. In particular, maxillary ante-rior teeth can shift lingually, mandibular anterior teeth can shift labially, and posterior cross bite and spacing can form randomly. In order to decrease the possibility of tooth movement and shift, an AM aligner is fabricated during the insertion visit. The periodontal health of the teeth, as well as original orthodon-tic bite classification are good indi-cators of bite relapse and can be a predict of the future results. Minor jaw ache and TMJ problem can develop during wearing the appli-ance. If these symptoms persist, the patient should stop wearing the appliance and adjustments should be made accordingly. The American Association of Dental Sleep Medicine 51 recommends using a consent form that informs the patients of possible side effects and risk factors of wearing MADs. Fig. 3: Upper and lower arches. outcomes. Recognizing the signs and symptoms of OSA and referring to a sleep specialist can save lives. OSA remains an important clinical and public health challenge. Under-standing the pathophysiology and function of sleep can help in the diagnosis and treatment of OSA. Dentists have an important role in the recognition and treatment of OSA. Overall, MADs are a valuable addition/alternative to CPAP for treating OSA and dentists can add sleep therapy to their practice by participating in training courses in the field of Dental Sleep Medicine. In addition, the training and education of office staff is important to provid-ing comprehensive dental sleep medicine care. Dentists should strive to work closely with sleep physicians and ear-nose-throat clinicians for patient referral. As members of this multi-disciplinary team, dentists can contribute to saving patient lives while treating OSA. 3. Tietjens JR, Claman D, Kezirian EJ, et al. Obstructive sleep apnea in cardiovascular disease: A review of the literature and proposed multidisciplinary clinical management strategy. J Am Heart Assoc. 2019;8(1). doi:10.1161/JAHA.118.010440 4. Braley TJ, Dunietz GL, Chervin RD, Lisa-beth LD, Skolarus LE, Burke JF. Recogni-tion and Diagnosis of Obstructive Sleep Apnea in Older Americans. J Am Geriatr Soc. 2018;66(7). doi:10.1111/jgs.15372 5. Mander BA, Winer JR, Walker MP. Sleep and Human Aging. Neuron. 2017;94(1). doi:10.1016/j.neuron.2017.02.004 6. Fuller PM, Gooley JJ, Saper CB. Neurobi-ology of the sleep-wake cycle: Sleep archi-tecture, circadian regulation, and regula-tory feedback. J Biol Rhythms. 2006;21(6).doi:10.1177/07487304062946 27 7. Hoekema A, Stegenga B, Wijkstra PJ, Van Der Hoeven JH, Meinesz AF, De Bont LGM. Obstructive sleep apnea therapy. J Dent Res. 2008;87(9). doi:10.1177/154405910808700917 8. Eckert DJ, Malhotra A, Jordan AS. Mecha-nisms of Apnea. Prog Cardiovasc Dis. 2009;51(4).doi:10.1016/j.pcad.2008.02.003 9. Jean-Louis G, Zizi F, Clark LT, Brown CD, McFarlane SI. Obstructive sleep apnea and cardiovascular disease: Role of the metabolic syndrome and its components. J Clin Sleep Med. 2008;4(3). doi:10.5664/jcsm.27191 10. Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2). doi:10.1513/pats.200707-114MG 11. Verbraecken JA, De Backer WA. Upper airway mechanics. Respiration. 2009;78(2). doi:10.1159/000222508 12. Aguilar M, Bhuket T, Torres S, Liu B, Wong RJ. Prevalence of the metabolic syndrome in the United States, 2003-Referring the Patient Back to the Sleep Physician After sufficient titration and improvement of sleep in conjunc-tion with subjective symptoms, including snoring and daytime sleepiness, the patient is referred back to the sleep physician for a sleep test with the MAD. This test will tell us if further advancement of the appliance is necessary. If the results are favorable, the patient is placed on a yearly recall. How Can Dentists Add Sleep Therapy to Their Practice The first step in adding sleep therapy to any dental practice is training. Taking basic courses followed by subsequent comprehen-sive courses in the field of Sleep Therapy can help dentists recognize the signs and symptoms of patients who might have OSA. Sleep evalua-tion should be part of any dentist’s treatment plan. We can train our hygienists and dental assistants to help to facilitate this process. Build-ing a good rapport and communi-cating with our fellow sleep physi-cians will help with the training process and improve patient References 1. Benjafield A V., Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnea: a literature-based analysis. Lancet Respir Med. 2019;7(8). doi:10.1016/S2213-2600(19)30198-5 2. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9). doi:10.1093/aje/kws342 www.orthodontics.com Summer 2021 35
Journal of the American Orthodontic Society Summer 2021: Page 35