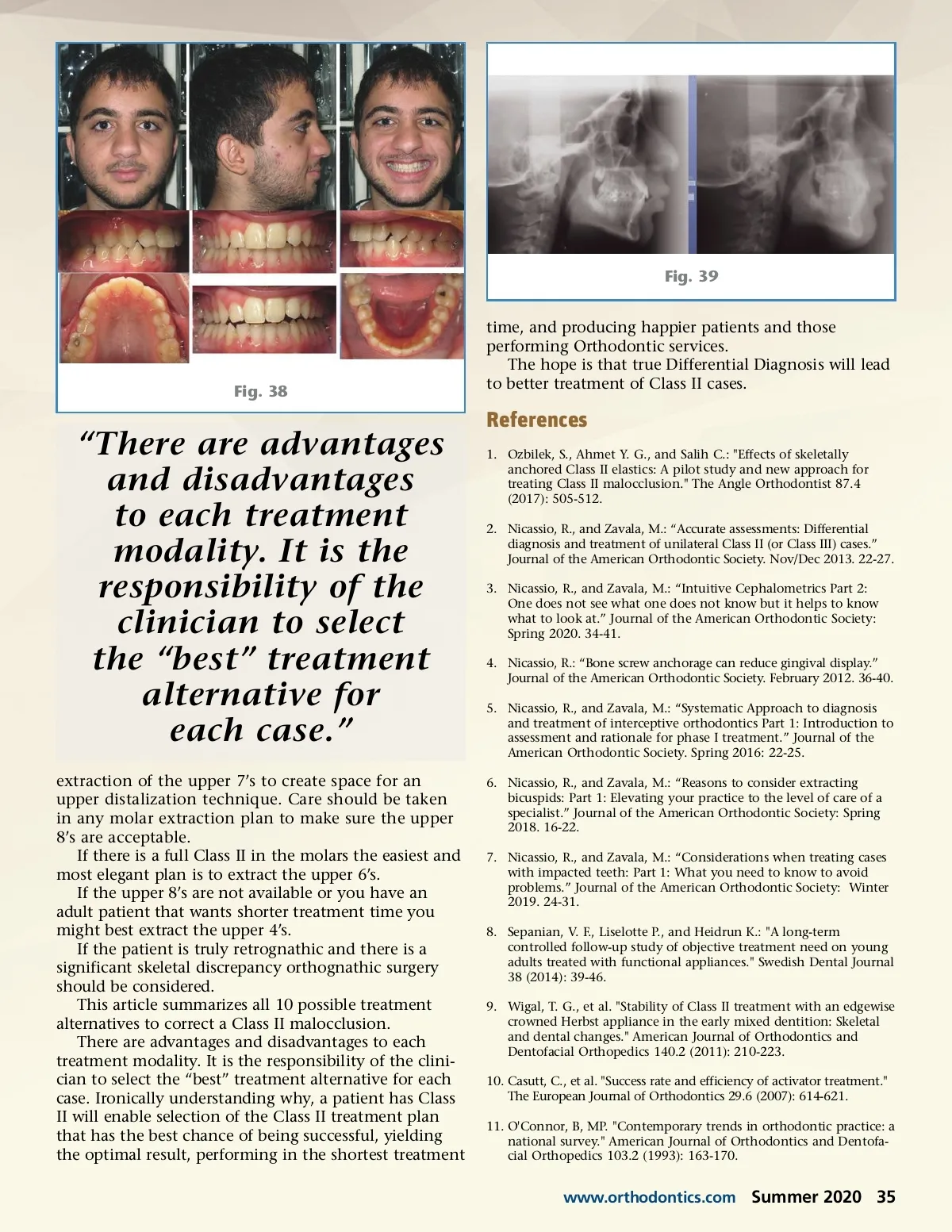
Fig. 39 time, and producing happier patients and those performing Orthodontic services. The hope is that true Differential Diagnosis will lead to better treatment of Class II cases. Fig. 38 “There are advantages and disadvantages to each treatment modality. It is the responsibility of the clinician to select the “best” treatment alternative for each case.” extraction of the upper 7’s to create space for an upper distalization technique. Care should be taken in any molar extraction plan to make sure the upper 8’s are acceptable. If there is a full Class II in the molars the easiest and most elegant plan is to extract the upper 6’s. If the upper 8’s are not available or you have an adult patient that wants shorter treatment time you might best extract the upper 4’s. If the patient is truly retrognathic and there is a significant skeletal discrepancy orthognathic surgery should be considered. This article summarizes all 10 possible treatment alternatives to correct a Class II malocclusion. There are advantages and disadvantages to each treatment modality. It is the responsibility of the clini-cian to select the “best” treatment alternative for each case. Ironically understanding why, a patient has Class II will enable selection of the Class II treatment plan that has the best chance of being successful, yielding the optimal result, performing in the shortest treatment References 1. Ozbilek, S., Ahmet Y. G., and Salih C.: "Effects of skeletally anchored Class II elastics: A pilot study and new approach for treating Class II malocclusion." The Angle Orthodontist 87.4 (2017): 505-512. 2. Nicassio, R., and Zavala, M.: “Accurate assessments: Differential diagnosis and treatment of unilateral Class II (or Class III) cases.” Journal of the American Orthodontic Society. Nov/Dec 2013. 22-27. 3. Nicassio, R., and Zavala, M.: “Intuitive Cephalometrics Part 2: One does not see what one does not know but it helps to know what to look at.” Journal of the American Orthodontic Society: Spring 2020. 34-41. 4. Nicassio, R.: “Bone screw anchorage can reduce gingival display.” Journal of the American Orthodontic Society. February 2012. 36-40. 5. Nicassio, R., and Zavala, M.: “Systematic Approach to diagnosis and treatment of interceptive orthodontics Part 1: Introduction to assessment and rationale for phase I treatment.” Journal of the American Orthodontic Society. Spring 2016: 22-25. 6. Nicassio, R., and Zavala, M.: “Reasons to consider extracting bicuspids: Part 1: Elevating your practice to the level of care of a specialist.” Journal of the American Orthodontic Society: Spring 2018. 16-22. 7. Nicassio, R., and Zavala, M.: “Considerations when treating cases with impacted teeth: Part 1: What you need to know to avoid problems.” Journal of the American Orthodontic Society: Winter 2019. 24-31. 8. Sepanian, V. F., Liselotte P., and Heidrun K.: "A long-term controlled follow-up study of objective treatment need on young adults treated with functional appliances." Swedish Dental Journal 38 (2014): 39-46. 9. Wigal, T. G., et al. "Stability of Class II treatment with an edgewise crowned Herbst appliance in the early mixed dentition: Skeletal and dental changes." American Journal of Orthodontics and Dentofacial Orthopedics 140.2 (2011): 210-223. 10. Casutt, C., et al. "Success rate and efficiency of activator treatment." The European Journal of Orthodontics 29.6 (2007): 614-621. 11. O'Connor, B, MP. "Contemporary trends in orthodontic practice: a national survey." American Journal of Orthodontics and Dentofa-cial Orthopedics 103.2 (1993): 163-170. www.orthodontics.com Summer 2020 35
Journal of the American Orthodontic Society Summer 2020: Page 35