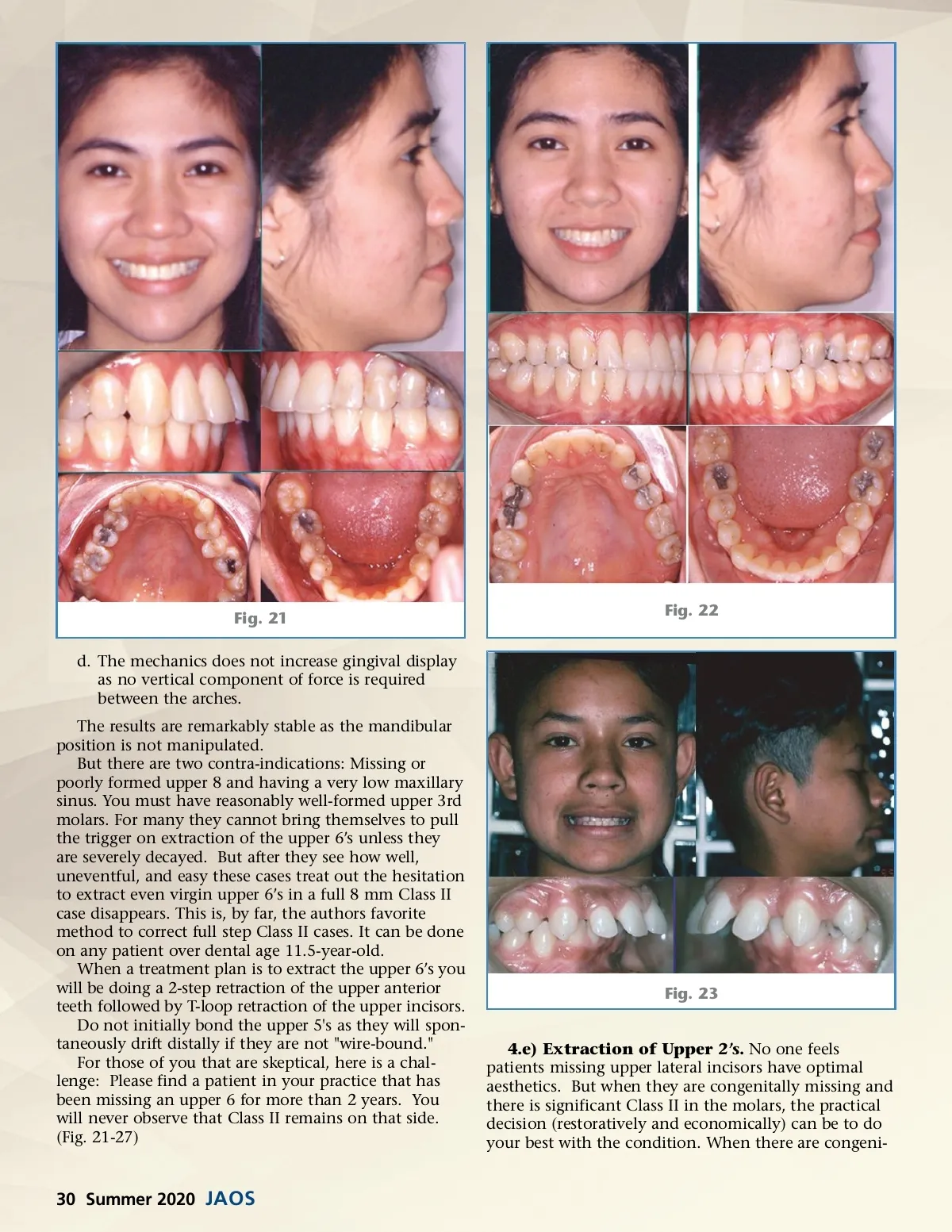
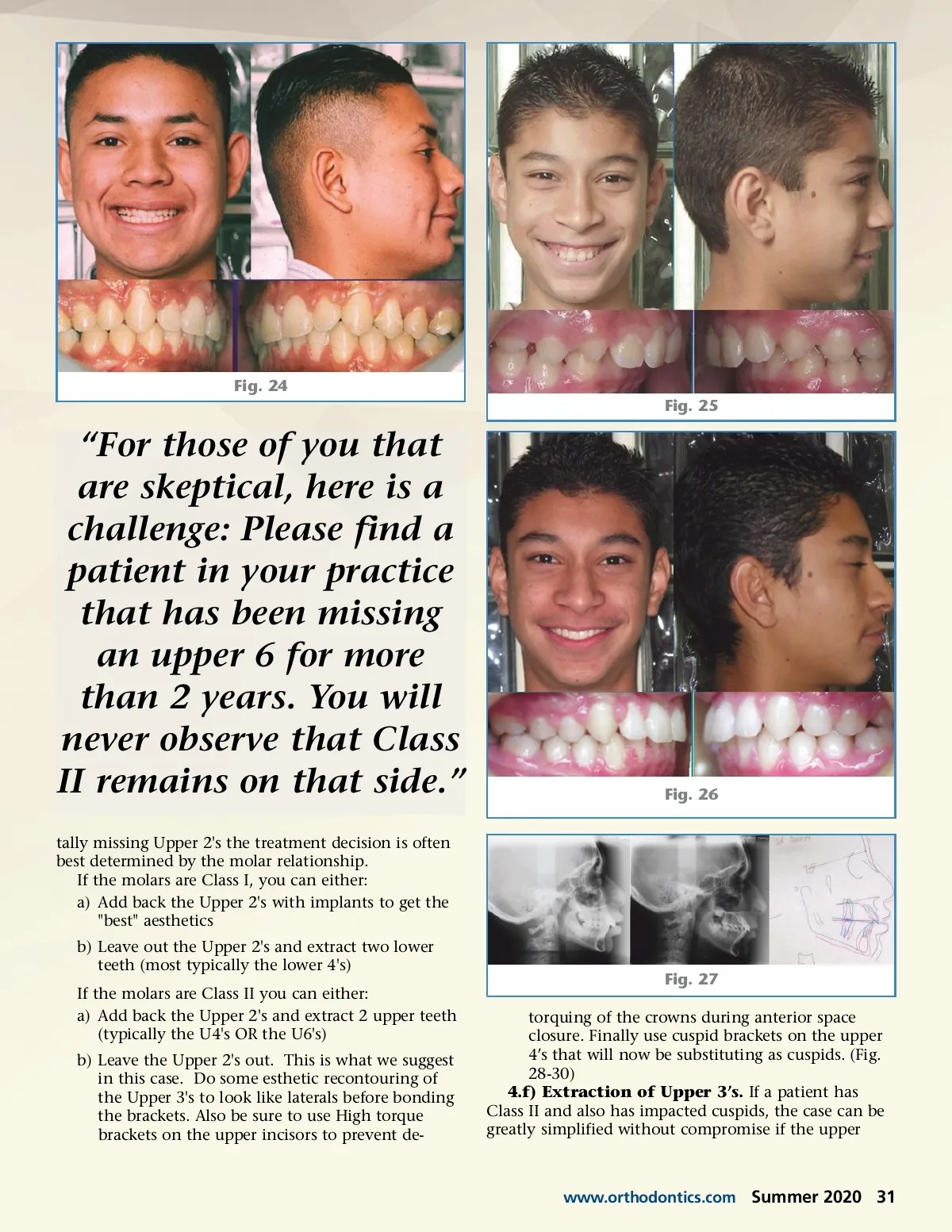
Fig. 21 d. The mechanics does not increase gingival display as no vertical component of force is required between the arches. The results are remarkably stable as the mandibular position is not manipulated. But there are two contra-indications: Missing or poorly formed upper 8 and having a very low maxillary sinus. You must have reasonably well-formed upper 3rd molars. For many they cannot bring themselves to pull the trigger on extraction of the upper 6’s unless they are severely decayed. But after they see how well, uneventful, and easy these cases treat out the hesitation to extract even virgin upper 6’s in a full 8 mm Class II case disappears. This is, by far, the authors favorite method to correct full step Class II cases. It can be done on any patient over dental age 11.5-year-old. When a treatment plan is to extract the upper 6’s you will be doing a 2-step retraction of the upper anterior teeth followed by T-loop retraction of the upper incisors. Do not initially bond the upper 5's as they will spon-taneously drift distally if they are not "wire-bound." For those of you that are skeptical, here is a chal-lenge: Please find a patient in your practice that has been missing an upper 6 for more than 2 years. You will never observe that Class II remains on that side. (Fig. 21-27) Fig. 22 Fig. 23 4.e) Extraction of Upper 2’s. No one feels patients missing upper lateral incisors have optimal aesthetics. But when they are congenitally missing and there is significant Class II in the molars, the practical decision (restoratively and economically) can be to do your best with the condition. When there are congeni-30 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 30