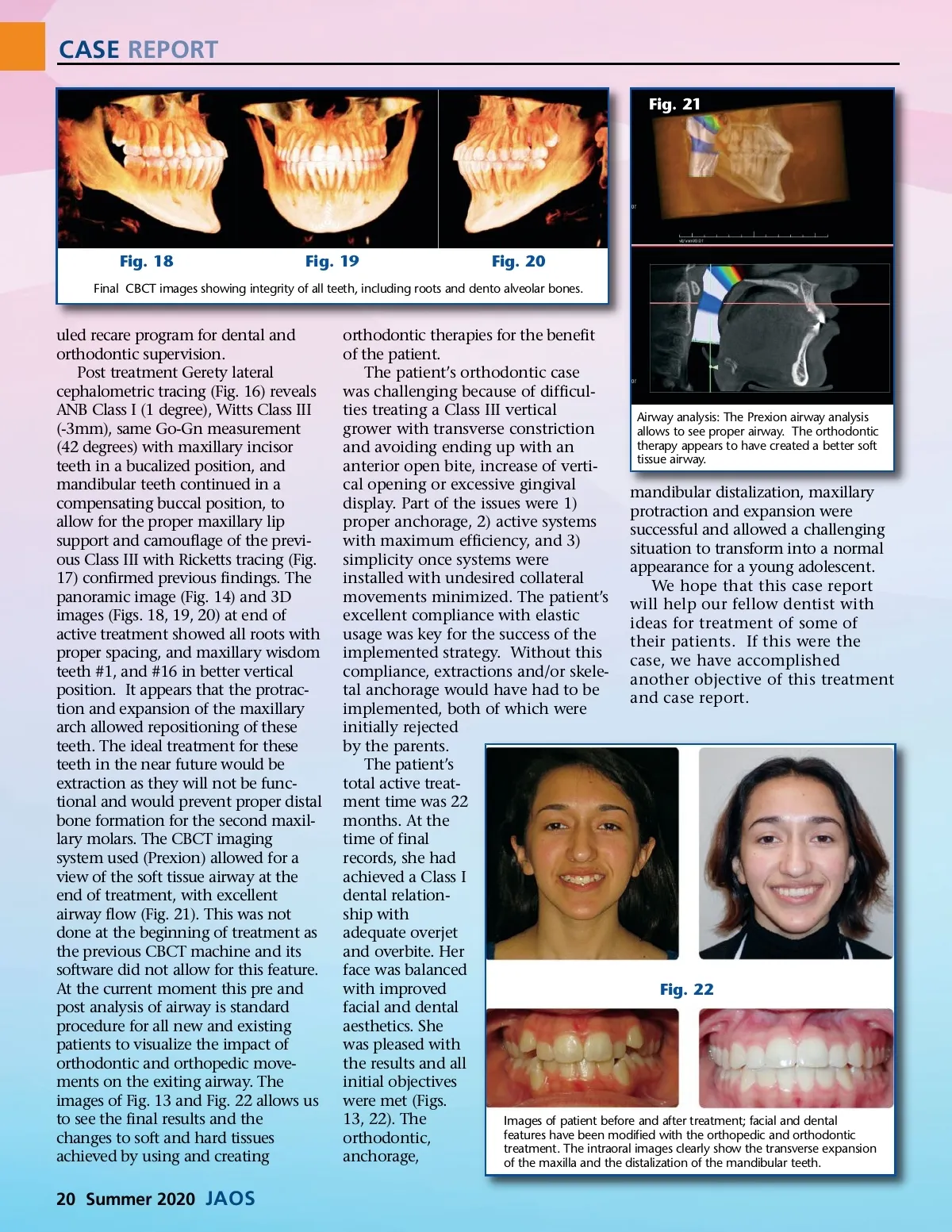
CASE REPORT Fig. 21 Fig. 18 Fig. 19 Fig. 20 Final CBCT images showing integrity of all teeth, including roots and dento alveolar bones. uled recare program for dental and orthodontic supervision. Post treatment Gerety lateral cephalometric tracing (Fig. 16) reveals ANB Class I (1 degree), Witts Class III (-3mm), same Go-Gn measurement (42 degrees) with maxillary incisor teeth in a bucalized position, and mandibular teeth continued in a compensating buccal position, to allow for the proper maxillary lip support and camouflage of the previ-ous Class III with Ricketts tracing (Fig. 17) confirmed previous findings. The panoramic image (Fig. 14) and 3D images (Figs. 18, 19, 20) at end of active treatment showed all roots with proper spacing, and maxillary wisdom teeth #1, and #16 in better vertical position. It appears that the protrac-tion and expansion of the maxillary arch allowed repositioning of these teeth. The ideal treatment for these teeth in the near future would be extraction as they will not be func-tional and would prevent proper distal bone formation for the second maxil-lary molars. The CBCT imaging system used (Prexion) allowed for a view of the soft tissue airway at the end of treatment, with excellent airway flow (Fig. 21). This was not done at the beginning of treatment as the previous CBCT machine and its software did not allow for this feature. At the current moment this pre and post analysis of airway is standard procedure for all new and existing patients to visualize the impact of orthodontic and orthopedic move-ments on the exiting airway. The images of Fig. 13 and Fig. 22 allows us to see the final results and the changes to soft and hard tissues achieved by using and creating orthodontic therapies for the benefit of the patient. The patient’s orthodontic case was challenging because of difficul-ties treating a Class III vertical Airway analysis: The Prexion airway analysis grower with transverse constriction allows to see proper airway. The orthodontic therapy appears to have created a better soft and avoiding ending up with an tissue airway. anterior open bite, increase of verti-cal opening or excessive gingival mandibular distalization, maxillary display. Part of the issues were 1) protraction and expansion were proper anchorage, 2) active systems successful and allowed a challenging with maximum efficiency, and 3) situation to transform into a normal simplicity once systems were appearance for a young adolescent. installed with undesired collateral We hope that this case report movements minimized. The patient’s will help our fellow dentist with excellent compliance with elastic ideas for treatment of some of usage was key for the success of the their patients. If this were the implemented strategy. Without this case, we have accomplished compliance, extractions and/or skele-another objective of this treatment tal anchorage would have had to be and case report. implemented, both of which were initially rejected by the parents. The patient’s total active treat-ment time was 22 months. At the time of final records, she had achieved a Class I dental relation-ship with adequate overjet and overbite. Her face was balanced with improved Fig. 22 facial and dental aesthetics. She was pleased with the results and all initial objectives were met (Figs. 13, 22). The Images of patient before and after treatment; facial and dental features have been modified with the orthopedic and orthodontic orthodontic, treatment. The intraoral images clearly show the transverse expansion anchorage, of the maxilla and the distalization of the mandibular teeth. 20 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 20