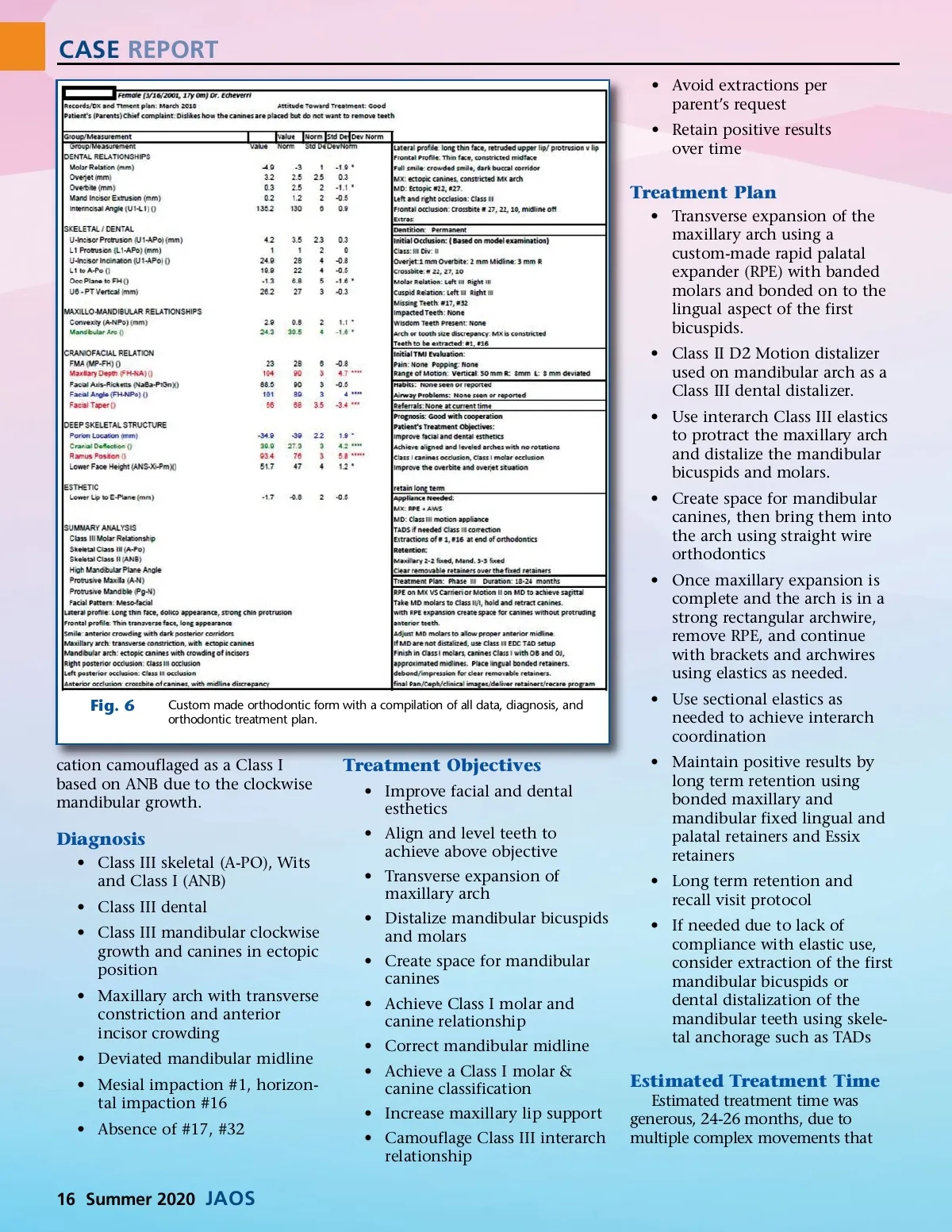
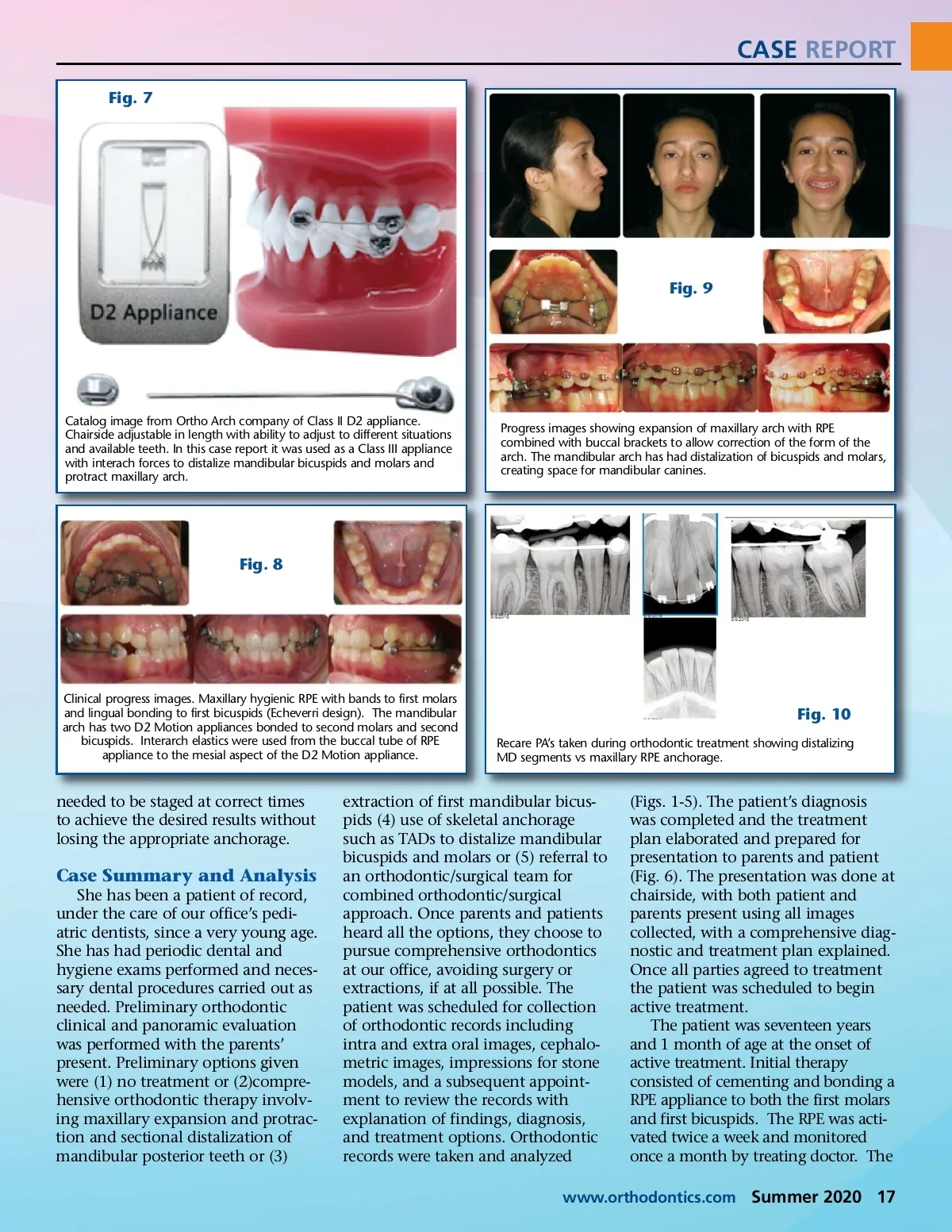
CASE REPORT Fig. 7 Fig. 9 Catalog image from Ortho Arch company of Class II D2 appliance. Chairside adjustable in length with ability to adjust to different situations and available teeth. In this case report it was used as a Class III appliance with interach forces to distalize mandibular bicuspids and molars and protract maxillary arch. Progress images showing expansion of maxillary arch with RPE combined with buccal brackets to allow correction of the form of the arch. The mandibular arch has had distalization of bicuspids and molars, creating space for mandibular canines. Fig. 8 Clinical progress images. Maxillary hygienic RPE with bands to first molars and lingual bonding to first bicuspids (Echeverri design). The mandibular arch has two D2 Motion appliances bonded to second molars and second bicuspids. Interarch elastics were used from the buccal tube of RPE appliance to the mesial aspect of the D2 Motion appliance. Fig. 10 Recare PA’s taken during orthodontic treatment showing distalizing MD segments vs maxillary RPE anchorage. needed to be staged at correct times to achieve the desired results without losing the appropriate anchorage. Case Summary and Analysis She has been a patient of record, under the care of our office’s pedi-atric dentists, since a very young age. She has had periodic dental and hygiene exams performed and neces-sary dental procedures carried out as needed. Preliminary orthodontic clinical and panoramic evaluation was performed with the parents’ present. Preliminary options given were (1) no treatment or (2)compre-hensive orthodontic therapy involv-ing maxillary expansion and protrac-tion and sectional distalization of mandibular posterior teeth or (3) extraction of first mandibular bicus-pids (4) use of skeletal anchorage such as TADs to distalize mandibular bicuspids and molars or (5) referral to an orthodontic/surgical team for combined orthodontic/surgical approach. Once parents and patients heard all the options, they choose to pursue comprehensive orthodontics at our office, avoiding surgery or extractions, if at all possible. The patient was scheduled for collection of orthodontic records including intra and extra oral images, cephalo-metric images, impressions for stone models, and a subsequent appoint-ment to review the records with explanation of findings, diagnosis, and treatment options. Orthodontic records were taken and analyzed (Figs. 1-5). The patient’s diagnosis was completed and the treatment plan elaborated and prepared for presentation to parents and patient (Fig. 6). The presentation was done at chairside, with both patient and parents present using all images collected, with a comprehensive diag-nostic and treatment plan explained. Once all parties agreed to treatment the patient was scheduled to begin active treatment. The patient was seventeen years and 1 month of age at the onset of active treatment. Initial therapy consisted of cementing and bonding a RPE appliance to both the first molars and first bicuspids. The RPE was acti-vated twice a week and monitored once a month by treating doctor. The www.orthodontics.com Summer 2020 17
Journal of the American Orthodontic Society Summer 2020: Page 17