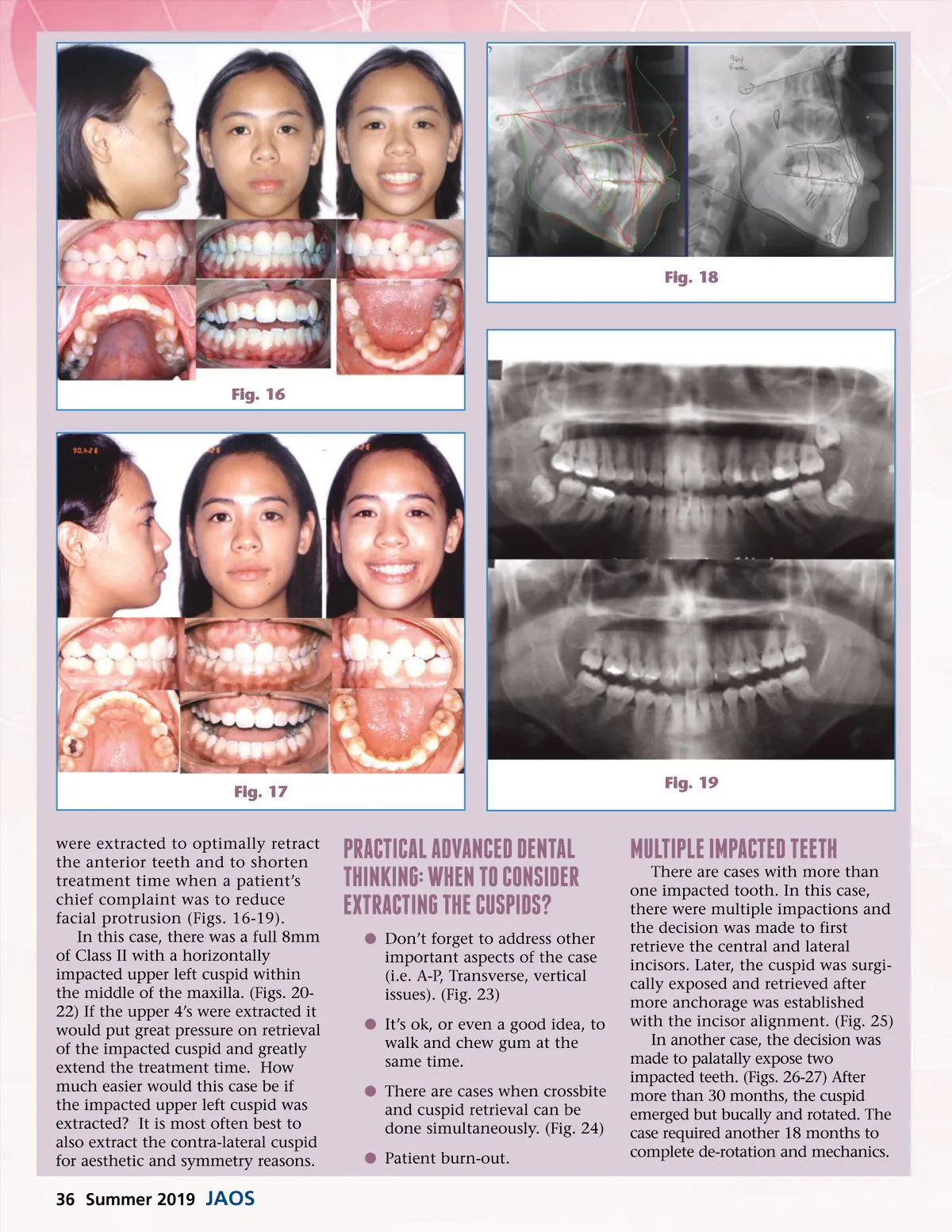
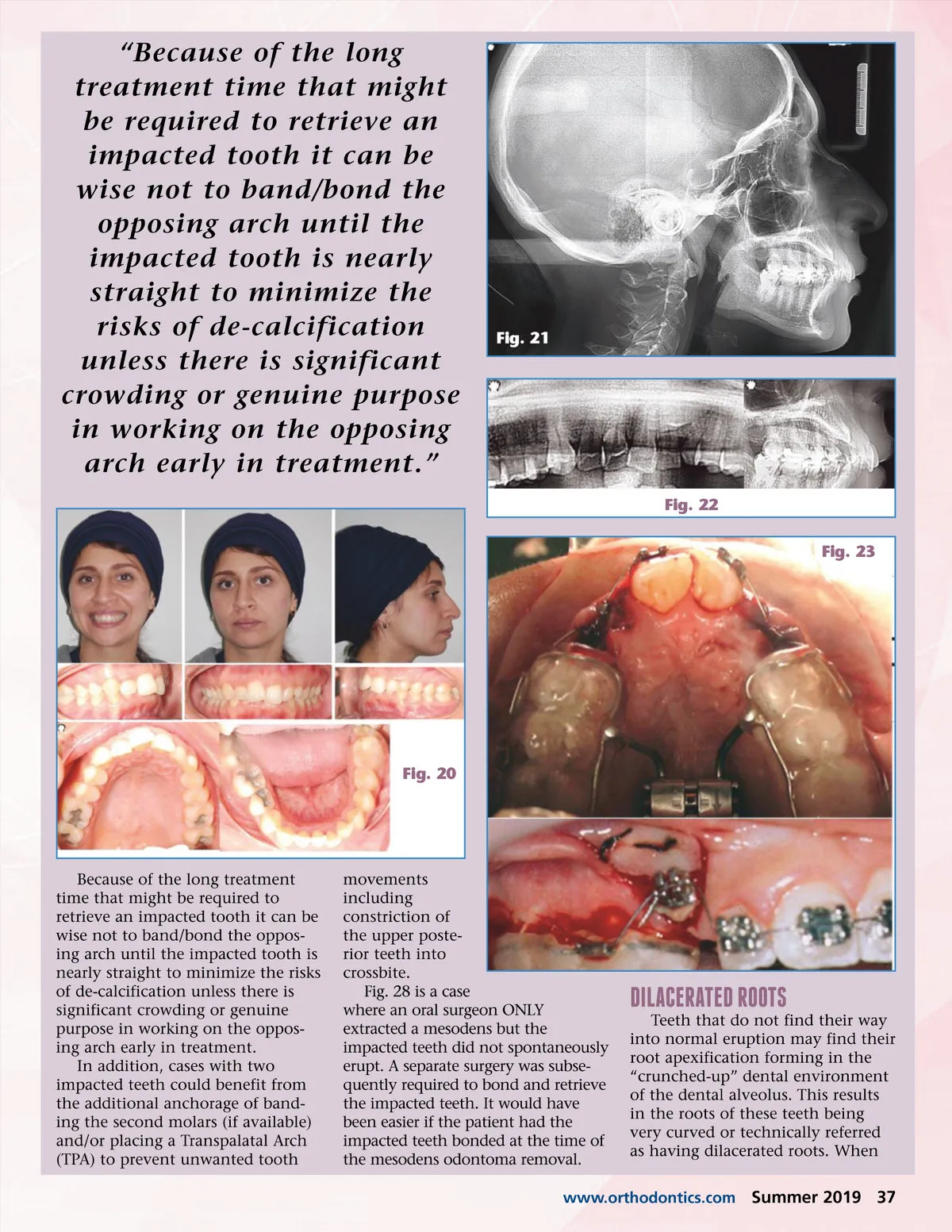
Fig. 18 Fig. 16 Fig. 17 were extracted to optimally retract the anterior teeth and to shorten treatment time when a patient’s chief complaint was to reduce facial protrusion (Figs. 16-19). In this case, there was a full 8mm of Class II with a horizontally impacted upper left cuspid within the middle of the maxilla. (Figs. 20-22) If the upper 4’s were extracted it would put great pressure on retrieval of the impacted cuspid and greatly extend the treatment time. How much easier would this case be if the impacted upper left cuspid was extracted? It is most often best to also extract the contra-lateral cuspid for aesthetic and symmetry reasons. Fig. 19 practIcal advanced dental thInkIng: When to consIder extractIng the cuspIds? b Don’t forget to address other important aspects of the case (i.e. A-P, Transverse, vertical issues). (Fig. 23) b It’s ok, or even a good idea, to walk and chew gum at the same time. b There are cases when crossbite and cuspid retrieval can be done simultaneously. (Fig. 24) b Patient burn-out. multIple Impacted teeth There are cases with more than one impacted tooth. In this case, there were multiple impactions and the decision was made to first retrieve the central and lateral incisors. Later, the cuspid was surgi-cally exposed and retrieved after more anchorage was established with the incisor alignment. (Fig. 25) In another case, the decision was made to palatally expose two impacted teeth. (Figs. 26-27) After more than 30 months, the cuspid emerged but bucally and rotated. The case required another 18 months to complete de-rotation and mechanics. 36 Summer 2019 JAOS
Journal of the American Orthodontic Society Summer 2019: Page 36