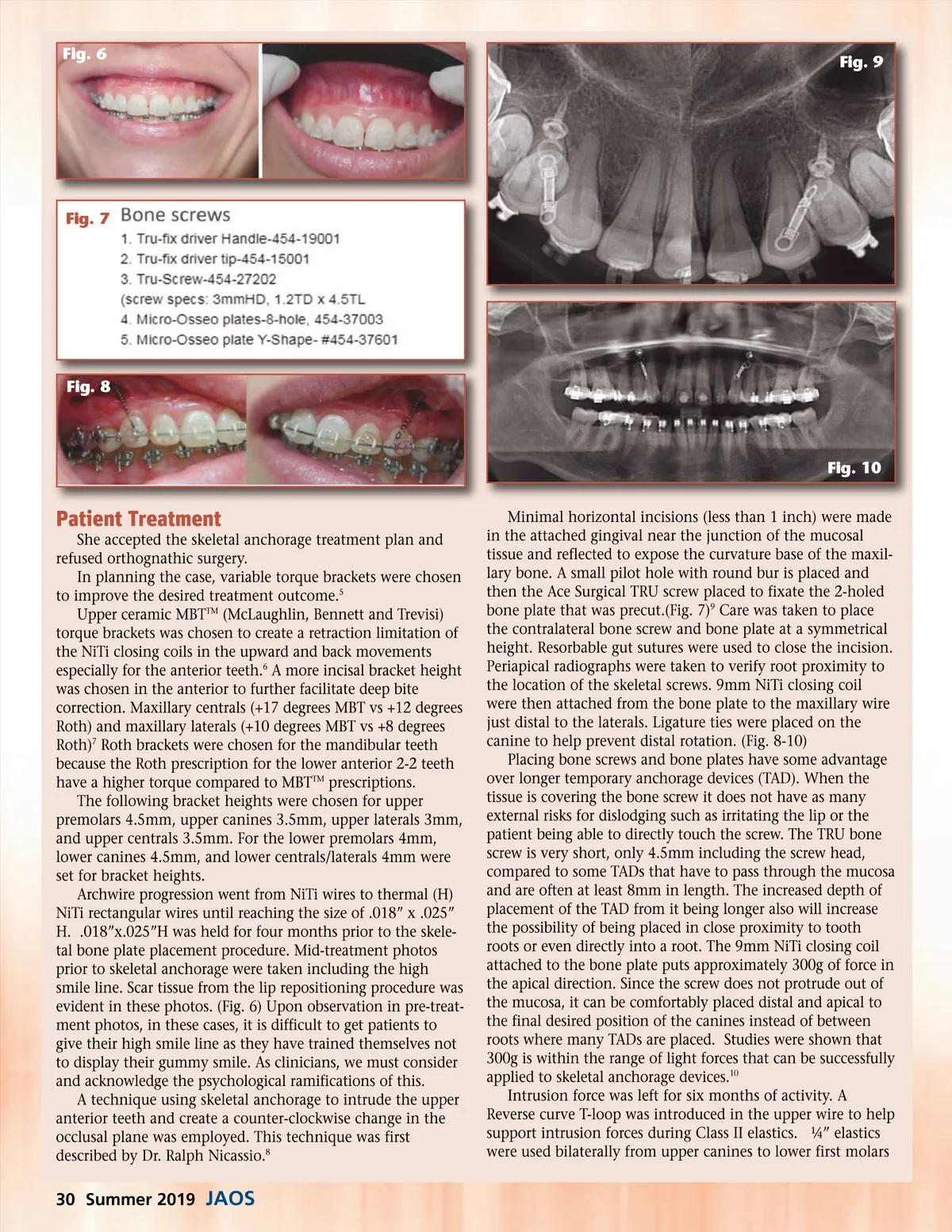
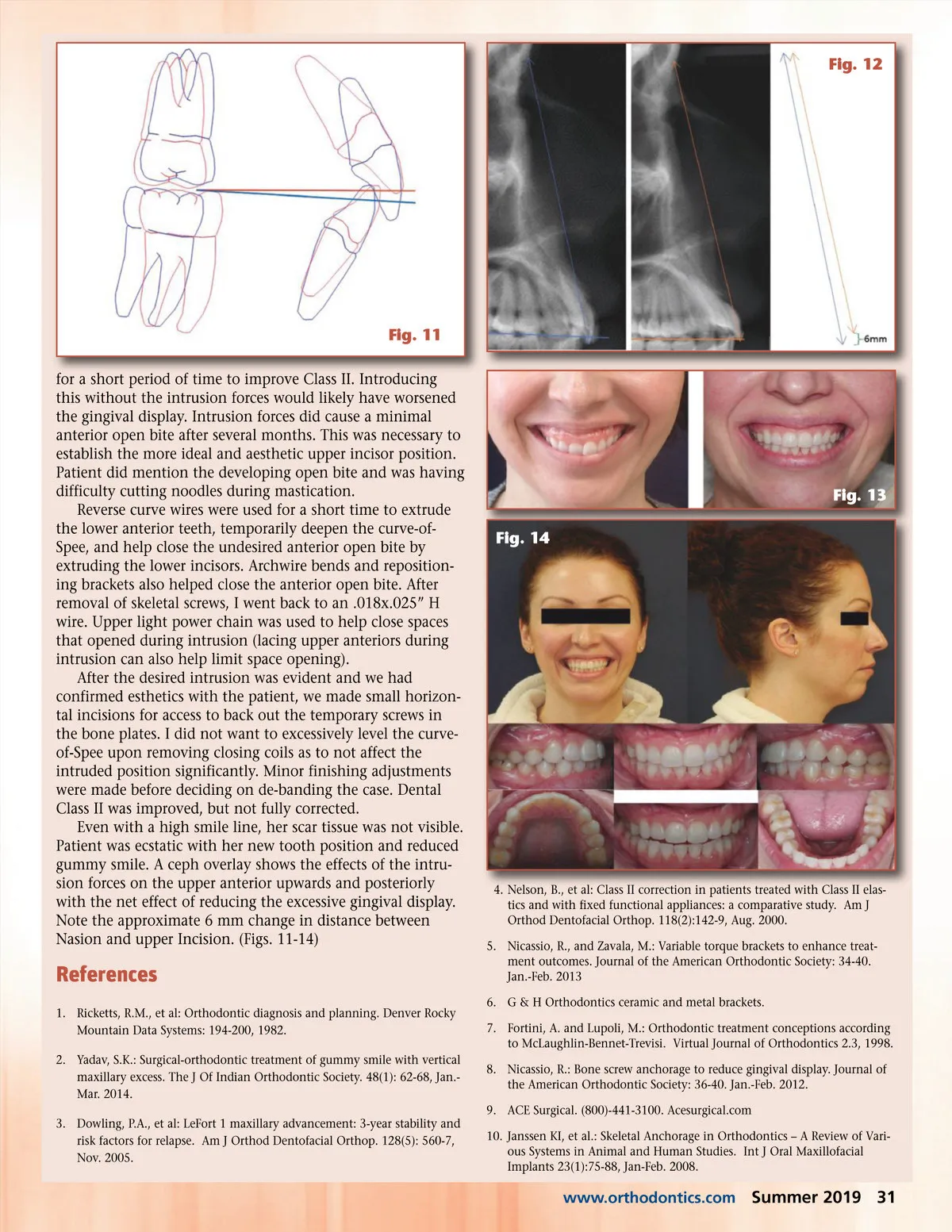
Fig. 12 Fig. 11 for a short period of time to improve Class II. Introducing this without the intrusion forces would likely have worsened the gingival display. Intrusion forces did cause a minimal anterior open bite after several months. This was necessary to establish the more ideal and aesthetic upper incisor position. Patient did mention the developing open bite and was having difficulty cutting noodles during mastication. Reverse curve wires were used for a short time to extrude the lower anterior teeth, temporarily deepen the curve-of-Spee, and help close the undesired anterior open bite by extruding the lower incisors. Archwire bends and reposition-ing brackets also helped close the anterior open bite. After removal of skeletal screws, I went back to an .018x.025” H wire. Upper light power chain was used to help close spaces that opened during intrusion (lacing upper anteriors during intrusion can also help limit space opening). After the desired intrusion was evident and we had confirmed esthetics with the patient, we made small horizon-tal incisions for access to back out the temporary screws in the bone plates. I did not want to excessively level the curve-of-Spee upon removing closing coils as to not affect the intruded position significantly. Minor finishing adjustments were made before deciding on de-banding the case. Dental Class II was improved, but not fully corrected. Even with a high smile line, her scar tissue was not visible. Patient was ecstatic with her new tooth position and reduced gummy smile. A ceph overlay shows the effects of the intru-sion forces on the upper anterior upwards and posteriorly with the net effect of reducing the excessive gingival display. Note the approximate 6 mm change in distance between Nasion and upper Incision. (Figs. 11-14) Fig. 13 Fig. 14 4. Nelson, B., et al: Class II correction in patients treated with Class II elas-tics and with fixed functional appliances: a comparative study. Am J Orthod Dentofacial Orthop. 118(2):142-9, Aug. 2000. 5. Nicassio, R., and Zavala, M.: Variable torque brackets to enhance treat-ment outcomes. Journal of the American Orthodontic Society: 34-40. Jan.-Feb. 2013 6. G & H Orthodontics ceramic and metal brackets. 7. Fortini, A. and Lupoli, M.: Orthodontic treatment conceptions according to McLaughlin-Bennet-Trevisi. Virtual Journal of Orthodontics 2.3, 1998. 8. Nicassio, R.: Bone screw anchorage to reduce gingival display. Journal of the American Orthodontic Society: 36-40. Jan.-Feb. 2012. 9. ACE Surgical. (800)-441-3100. Acesurgical.com References 1. Ricketts, R.M., et al: Orthodontic diagnosis and planning. Denver Rocky Mountain Data Systems: 194-200, 1982. 2. Yadav, S.K.: Surgical-orthodontic treatment of gummy smile with vertical maxillary excess. The J Of Indian Orthodontic Society. 48(1): 62-68, Jan.-Mar. 2014. 3. Dowling, P.A., et al: LeFort 1 maxillary advancement: 3-year stability and risk factors for relapse. Am J Orthod Dentofacial Orthop. 128(5): 560-7, Nov. 2005. 10. Janssen KI, et al.: Skeletal Anchorage in Orthodontics – A Review of Vari-ous Systems in Animal and Human Studies. Int J Oral Maxillofacial Implants 23(1):75-88, Jan-Feb. 2008. www.orthodontics.com Summer 2019 31
Journal of the American Orthodontic Society Summer 2019: Page 31