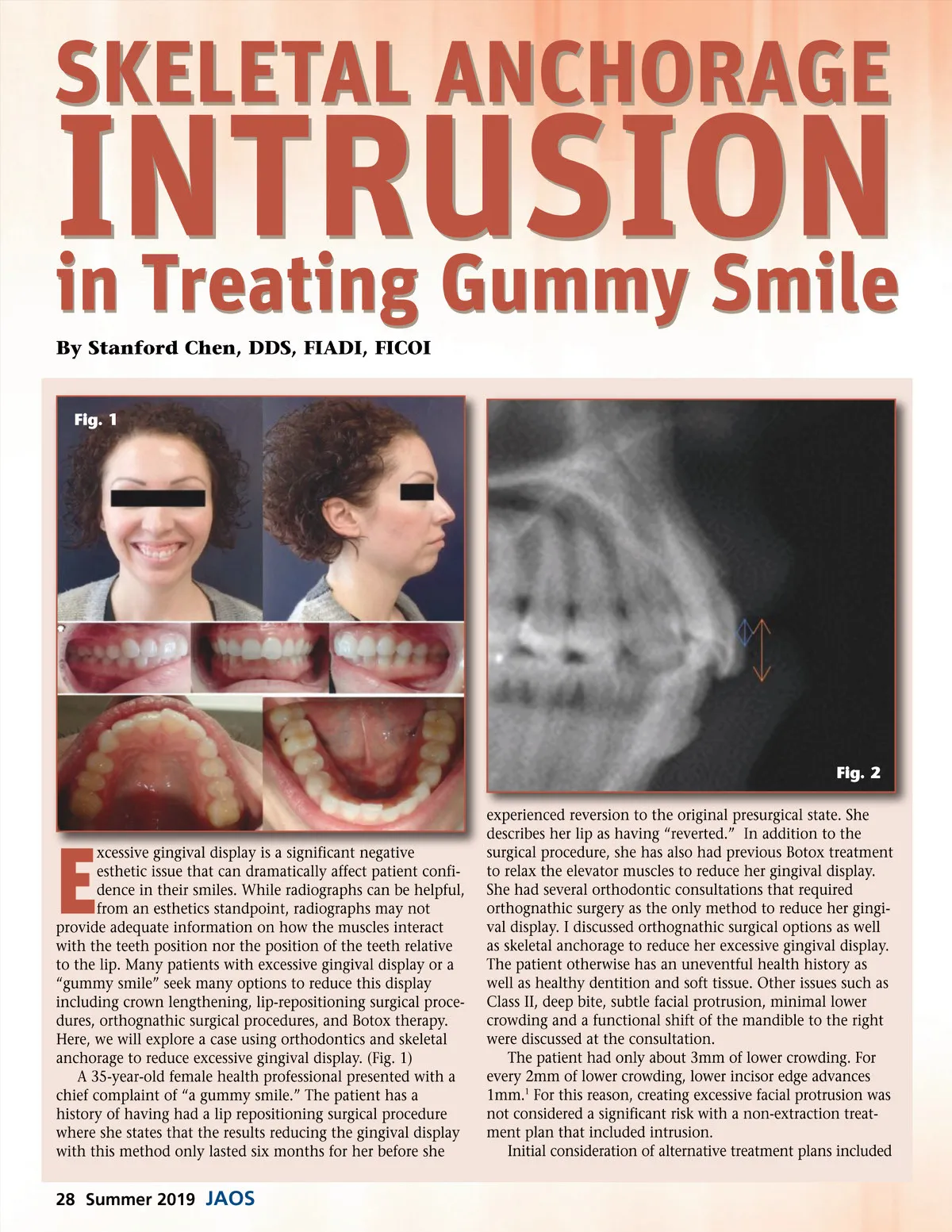
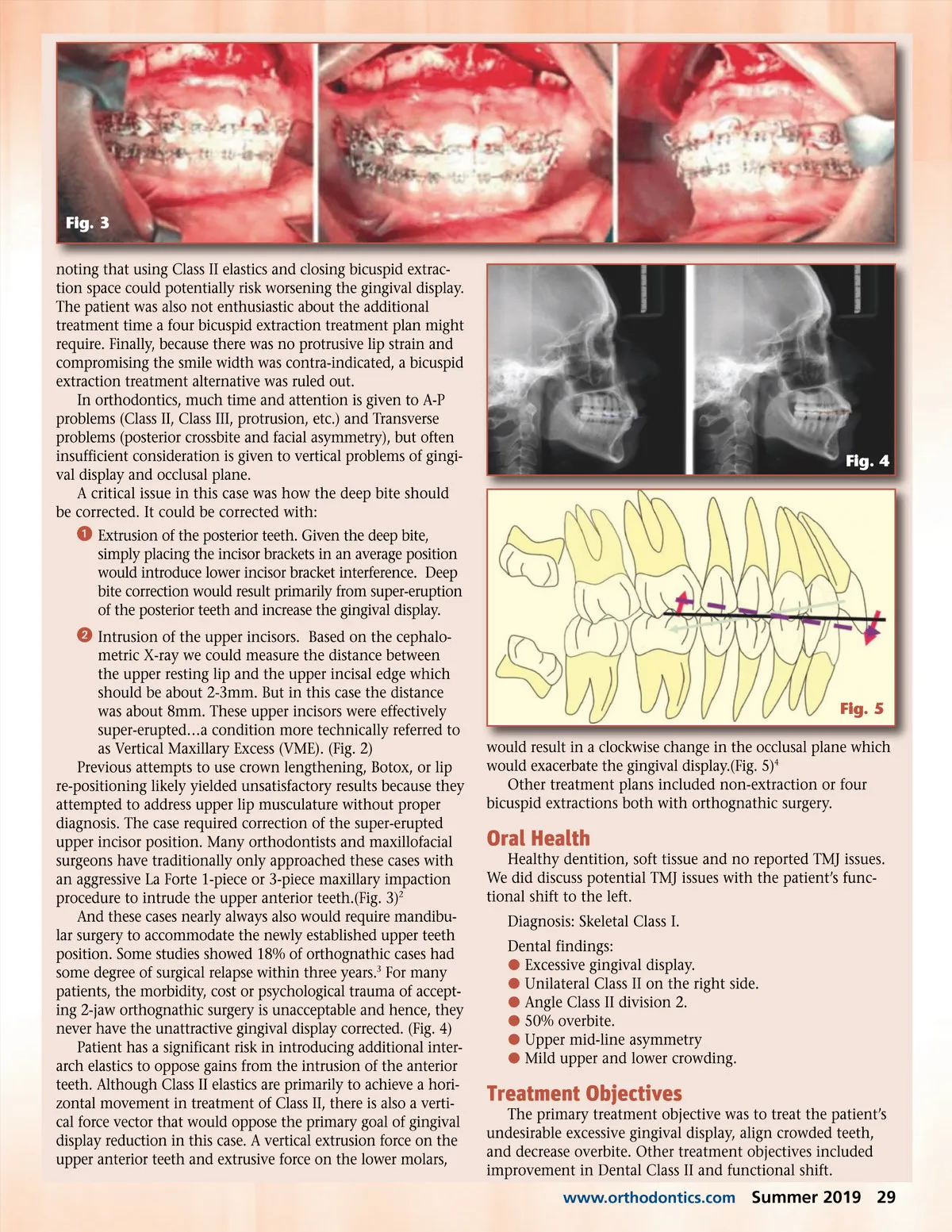
Fig. 3 noting that using Class II elastics and closing bicuspid extrac-tion space could potentially risk worsening the gingival display. The patient was also not enthusiastic about the additional treatment time a four bicuspid extraction treatment plan might require. Finally, because there was no protrusive lip strain and compromising the smile width was contra-indicated, a bicuspid extraction treatment alternative was ruled out. In orthodontics, much time and attention is given to A-P problems (Class II, Class III, protrusion, etc.) and Transverse problems (posterior crossbite and facial asymmetry), but often insufficient consideration is given to vertical problems of gingi-val display and occlusal plane. A critical issue in this case was how the deep bite should be corrected. It could be corrected with: ᕡ Extrusion of the posterior teeth. Given the deep bite, simply placing the incisor brackets in an average position would introduce lower incisor bracket interference. Deep bite correction would result primarily from super-eruption of the posterior teeth and increase the gingival display. ᕢ Intrusion of the upper incisors. Based on the cephalo-metric X-ray we could measure the distance between the upper resting lip and the upper incisal edge which should be about 2-3mm. But in this case the distance was about 8mm. These upper incisors were effectively super-erupted…a condition more technically referred to as Vertical Maxillary Excess (VME). (Fig. 2) Previous attempts to use crown lengthening, Botox, or lip re-positioning likely yielded unsatisfactory results because they attempted to address upper lip musculature without proper diagnosis. The case required correction of the super-erupted upper incisor position. Many orthodontists and maxillofacial surgeons have traditionally only approached these cases with an aggressive La Forte 1-piece or 3-piece maxillary impaction procedure to intrude the upper anterior teeth.(Fig. 3) 2 And these cases nearly always also would require mandibu-lar surgery to accommodate the newly established upper teeth position. Some studies showed 18% of orthognathic cases had some degree of surgical relapse within three years. 3 For many patients, the morbidity, cost or psychological trauma of accept-ing 2-jaw orthognathic surgery is unacceptable and hence, they never have the unattractive gingival display corrected. (Fig. 4) Patient has a significant risk in introducing additional inter-arch elastics to oppose gains from the intrusion of the anterior teeth. Although Class II elastics are primarily to achieve a hori-zontal movement in treatment of Class II, there is also a verti-cal force vector that would oppose the primary goal of gingival display reduction in this case. A vertical extrusion force on the upper anterior teeth and extrusive force on the lower molars, Fig. 4 Fig. 5 would result in a clockwise change in the occlusal plane which would exacerbate the gingival display.(Fig. 5) 4 Other treatment plans included non-extraction or four bicuspid extractions both with orthognathic surgery. Oral Health Healthy dentition, soft tissue and no reported TMJ issues. We did discuss potential TMJ issues with the patient’s func-tional shift to the left. Diagnosis: Skeletal Class I. Dental findings: b Excessive gingival display. b Unilateral Class II on the right side. b Angle Class II division 2. b 50% overbite. b Upper mid-line asymmetry b Mild upper and lower crowding. Treatment Objectives The primary treatment objective was to treat the patient’s undesirable excessive gingival display, align crowded teeth, and decrease overbite. Other treatment objectives included improvement in Dental Class II and functional shift. www.orthodontics.com Summer 2019 29
Journal of the American Orthodontic Society Summer 2019: Page 29