Early Class III Treatment: Is the Benefit Worth the Burden? By Leonard J. Carapezza, DMD even out of ten children will have developed a malocclusion by the time they have reached peak puberty. Ninety percent of these malocclusions are tooth related caused by environmental issues (eg. oral habits and medical induced mouth breathing). The remaining ten percent of developing pediatric malocclusions are skeletal-based caused by hereditary and neuromus-cular problems. These conditions can affect normal jaw growth and devel-opment in the Transverse, Horizon-tal and Vertical planes of cranio-facial growth. It is the goal of pedi-atric orthodontics to intercept and rectify abnormal growth patterns of the craniofacial structures. The clinical delivery of early orthodontic care in private pediatric practice does so in one of three ways: preferably Growth Modification , Camou-flage Treatment and delaying treatment with referral for Orthognathic Surgery when growth is completed. The Class III malocclusion is the most precarious to diagnose and treat because of the latent genetic potential and the differential growth patterns that may result. The author has reviewed the litera-ture and published a degree of diffi-culty classification of the Class III into seven sub-types. 1 (Table 1) S Fig. 1 Class III familial triplets, Age 4 Patients E.P. (L), J.P. (C), C.P. (R). Patient History A family of young healthy triplets -a male and two females, entered the clinician’s practice at the age of 2 ½. The medical and social history revealed the father and their pater-18 Summer 2019 JAOS
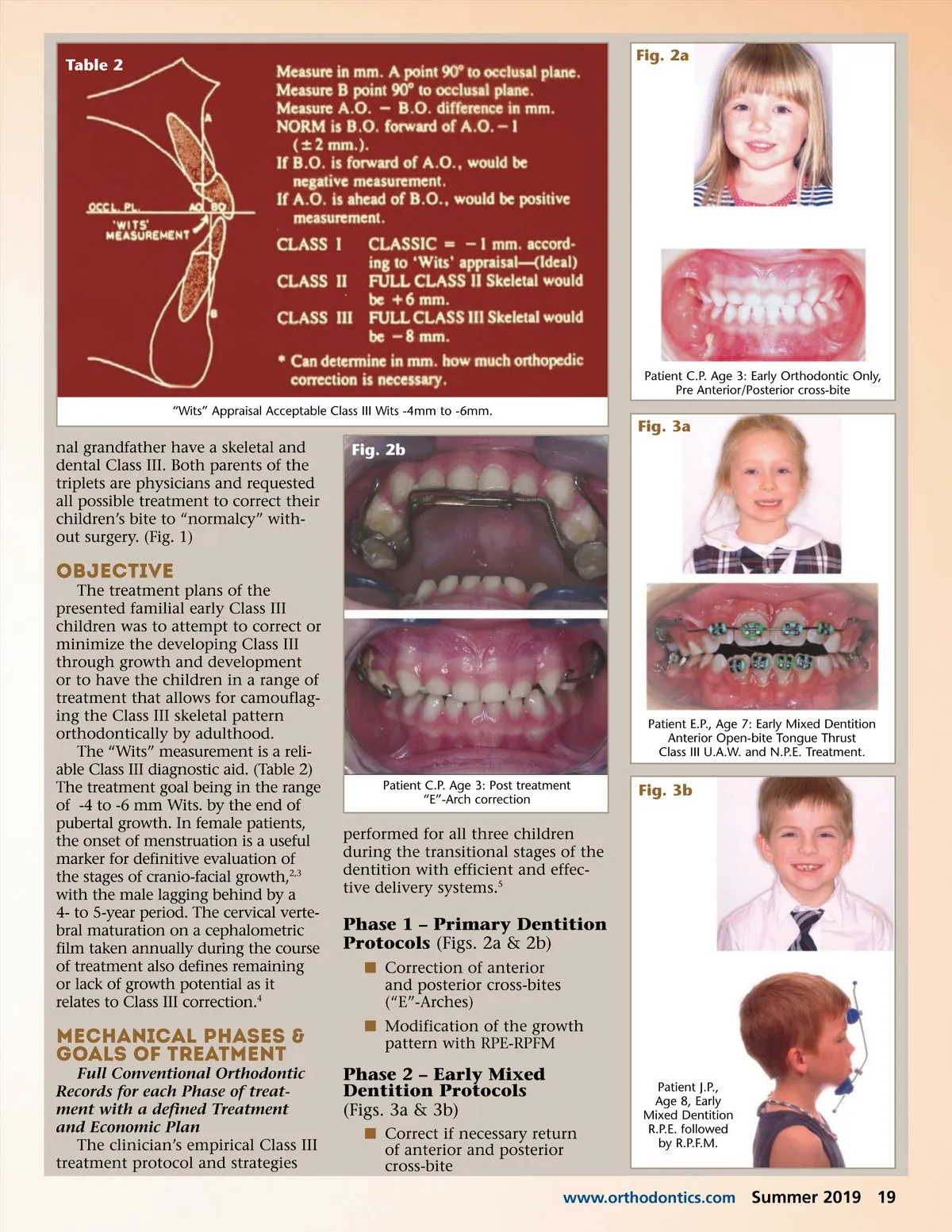
Journal of the American Orthodontic Society Summer 2019: Page 18