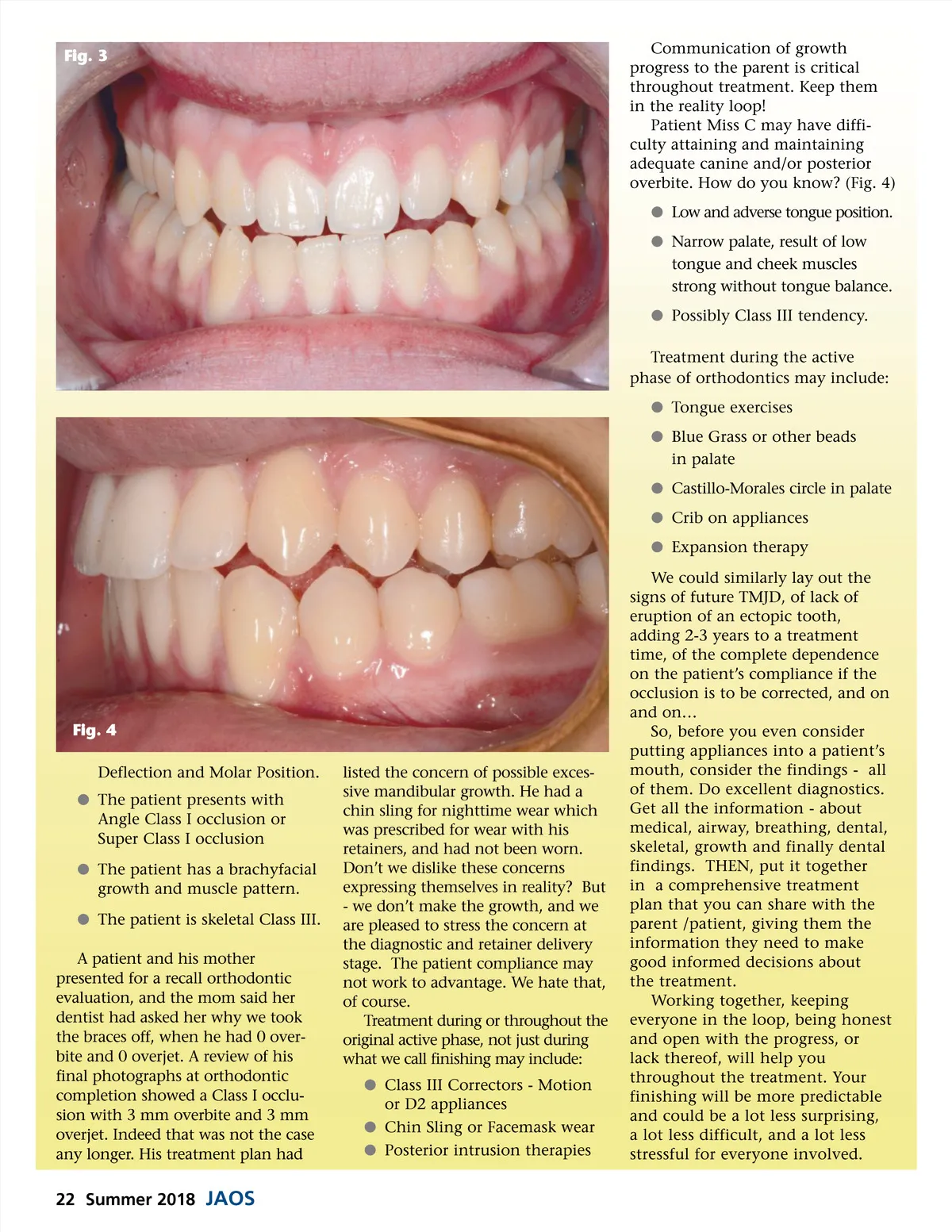
Fig. 3 Communication of growth progress to the parent is critical throughout treatment. Keep them in the reality loop! Patient Miss C may have diffi-culty attaining and maintaining adequate canine and/or posterior overbite. How do you know? (Fig. 4) b Low and adverse tongue position. b Narrow palate, result of low tongue and cheek muscles strong without tongue balance. b Possibly Class III tendency. Treatment during the active phase of orthodontics may include: b Tongue exercises b Blue Grass or other beads in palate b Castillo-Morales circle in palate b Crib on appliances b Expansion therapy We could similarly lay out the signs of future TMJD, of lack of eruption of an ectopic tooth, adding 2-3 years to a treatment time, of the complete dependence on the patient’s compliance if the occlusion is to be corrected, and on and on… So, before you even consider putting appliances into a patient’s mouth, consider the findings -all of them. Do excellent diagnostics. Get all the information -about medical, airway, breathing, dental, skeletal, growth and finally dental findings. THEN, put it together in a comprehensive treatment plan that you can share with the parent /patient, giving them the information they need to make good informed decisions about the treatment. Working together, keeping everyone in the loop, being honest and open with the progress, or lack thereof, will help you throughout the treatment. Your finishing will be more predictable and could be a lot less surprising, a lot less difficult, and a lot less stressful for everyone involved. Fig. 4 Deflection and Molar Position. b The patient presents with Angle Class I occlusion or Super Class I occlusion b The patient has a brachyfacial growth and muscle pattern. b The patient is skeletal Class III. A patient and his mother presented for a recall orthodontic evaluation, and the mom said her dentist had asked her why we took the braces off, when he had 0 over-bite and 0 overjet. A review of his final photographs at orthodontic completion showed a Class I occlu-sion with 3 mm overbite and 3 mm overjet. Indeed that was not the case any longer. His treatment plan had listed the concern of possible exces-sive mandibular growth. He had a chin sling for nighttime wear which was prescribed for wear with his retainers, and had not been worn. Don’t we dislike these concerns expressing themselves in reality? But -we don’t make the growth, and we are pleased to stress the concern at the diagnostic and retainer delivery stage. The patient compliance may not work to advantage. We hate that, of course. Treatment during or throughout the original active phase, not just during what we call finishing may include: b Class III Correctors -Motion or D2 appliances b Chin Sling or Facemask wear b Posterior intrusion therapies 22 Summer 2018 JAOS
Journal of the American Orthodontic Society Summer 2018/Buyer's Guide: Page 22