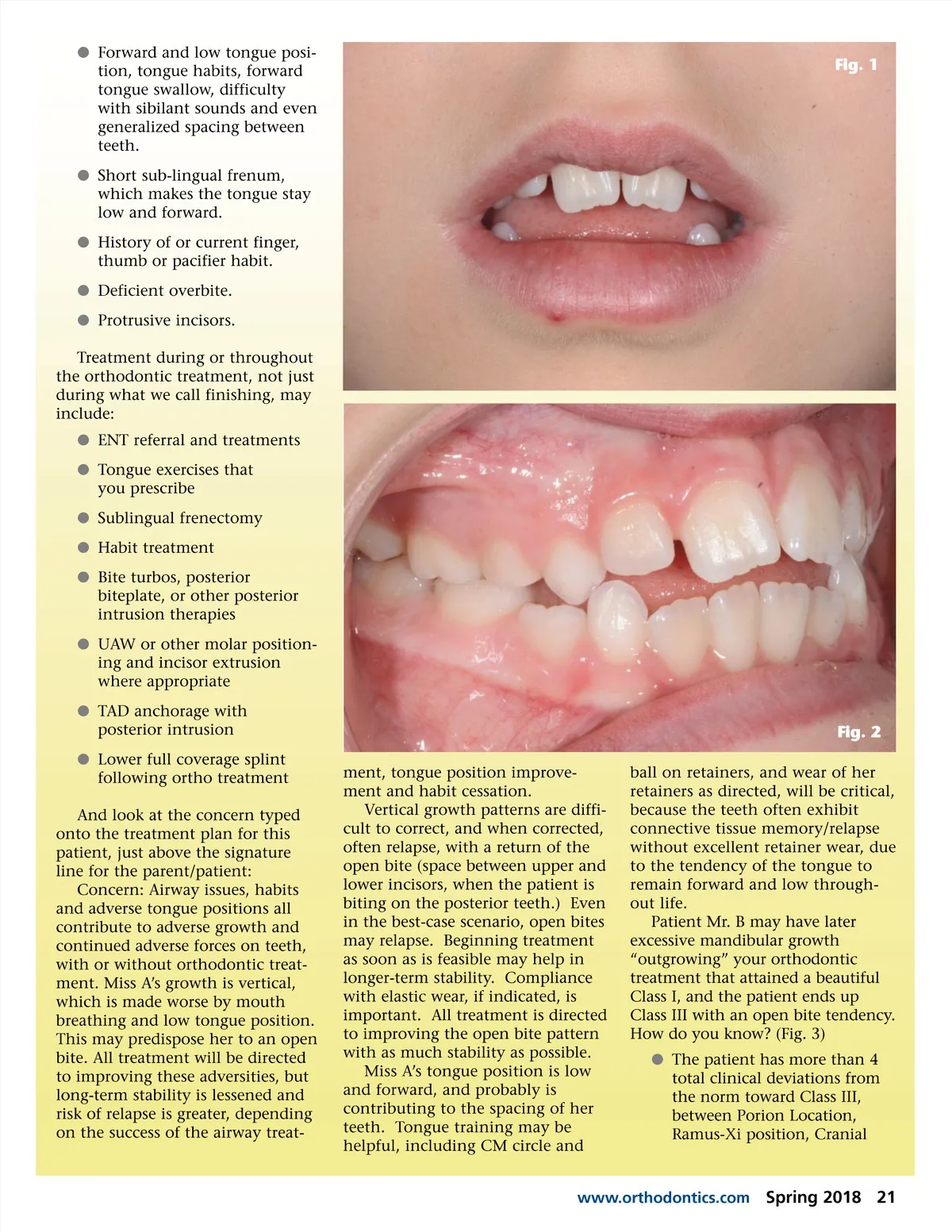
b Forward and low tongue posi-tion, tongue habits, forward tongue swallow, difficulty with sibilant sounds and even generalized spacing between teeth. b Short sub-lingual frenum, which makes the tongue stay low and forward. b History of or current finger, thumb or pacifier habit. b Deficient overbite. b Protrusive incisors. Treatment during or throughout the orthodontic treatment, not just during what we call finishing, may include: b ENT referral and treatments b Tongue exercises that you prescribe b Sublingual frenectomy b Habit treatment b Bite turbos, posterior biteplate, or other posterior intrusion therapies b UAW or other molar position-ing and incisor extrusion where appropriate b TAD anchorage with posterior intrusion b Lower full coverage splint following ortho treatment And look at the concern typed onto the treatment plan for this patient, just above the signature line for the parent/patient: Concern: Airway issues, habits and adverse tongue positions all contribute to adverse growth and continued adverse forces on teeth, with or without orthodontic treat-ment. Miss A’s growth is vertical, which is made worse by mouth breathing and low tongue position. This may predispose her to an open bite. All treatment will be directed to improving these adversities, but long-term stability is lessened and risk of relapse is greater, depending on the success of the airway treat-ment, tongue position improve-ment and habit cessation. Vertical growth patterns are diffi-cult to correct, and when corrected, often relapse, with a return of the open bite (space between upper and lower incisors, when the patient is biting on the posterior teeth.) Even in the best-case scenario, open bites may relapse. Beginning treatment as soon as is feasible may help in longer-term stability. Compliance with elastic wear, if indicated, is important. All treatment is directed to improving the open bite pattern with as much stability as possible. Miss A’s tongue position is low and forward, and probably is contributing to the spacing of her teeth. Tongue training may be helpful, including CM circle and Fig. 1 Fig. 2 ball on retainers, and wear of her retainers as directed, will be critical, because the teeth often exhibit connective tissue memory/relapse without excellent retainer wear, due to the tendency of the tongue to remain forward and low through-out life. Patient Mr. B may have later excessive mandibular growth “outgrowing” your orthodontic treatment that attained a beautiful Class I, and the patient ends up Class III with an open bite tendency. How do you know? (Fig. 3) b The patient has more than 4 total clinical deviations from the norm toward Class III, between Porion Location, Ramus-Xi position, Cranial www.orthodontics.com Spring 2018 21
Journal of the American Orthodontic Society Summer 2018/Buyer's Guide: Page 21