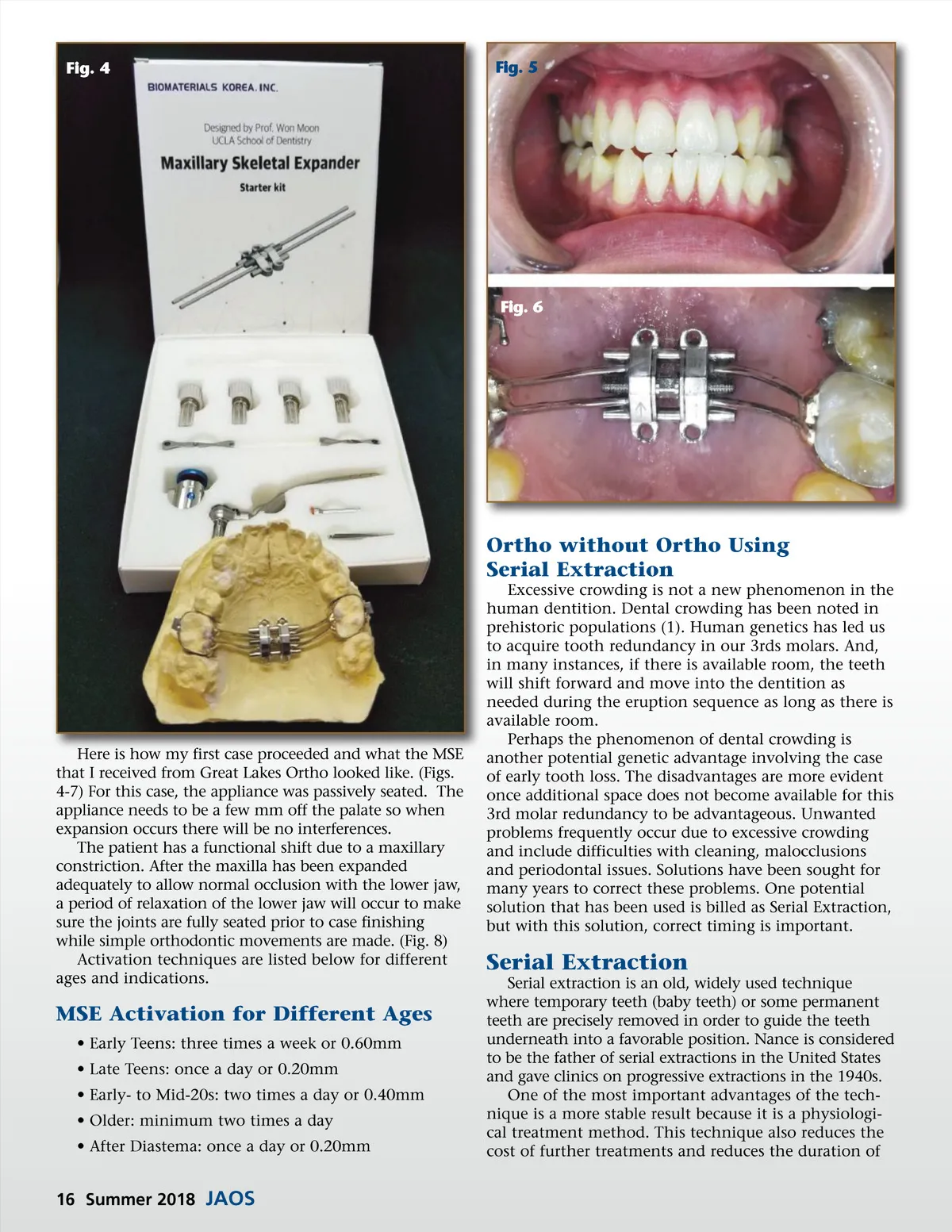
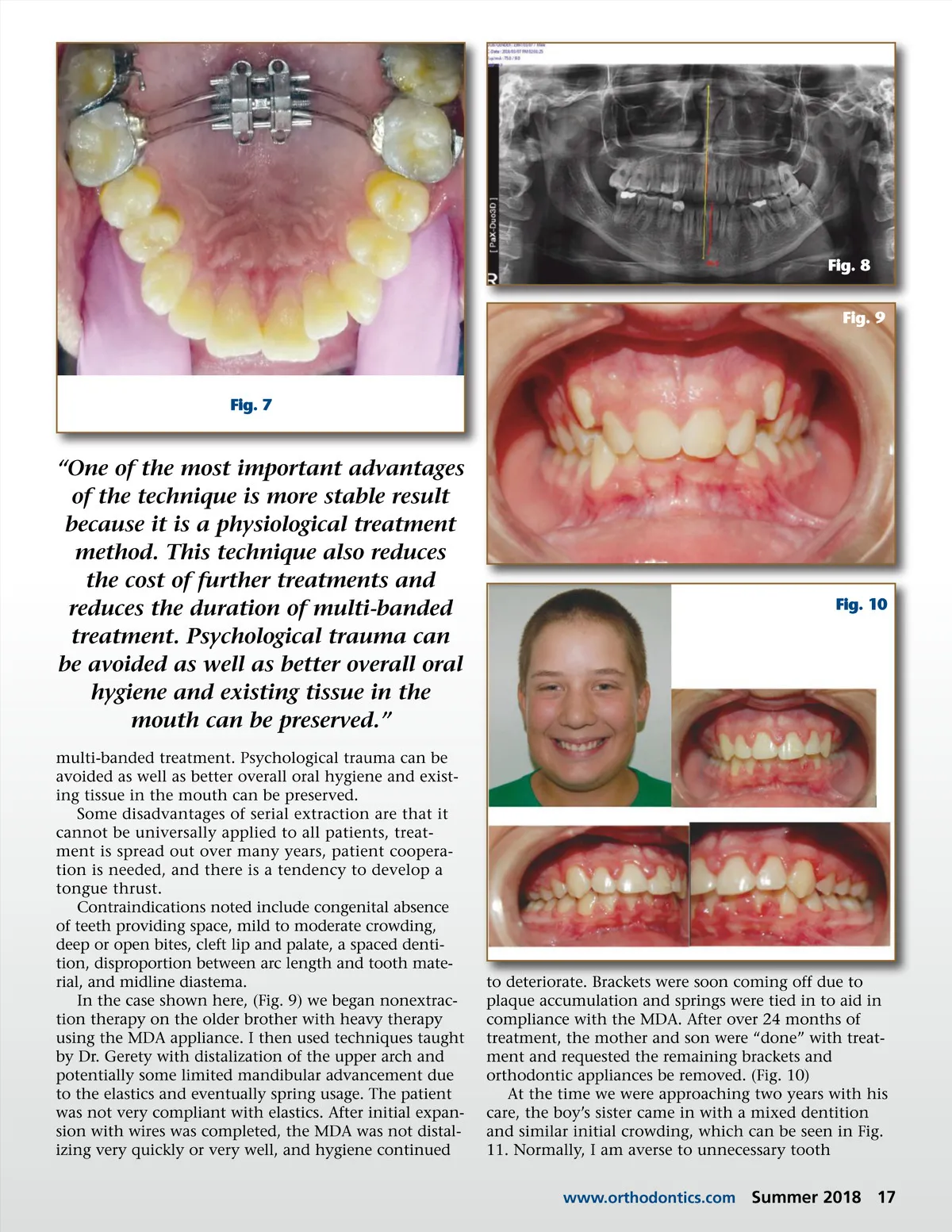
Fig. 8 Fig. 9 Fig. 7 “One of the most important advantages of the technique is more stable result because it is a physiological treatment method. This technique also reduces the cost of further treatments and reduces the duration of multi-banded treatment. Psychological trauma can be avoided as well as better overall oral hygiene and existing tissue in the mouth can be preserved.” multi-banded treatment. Psychological trauma can be avoided as well as better overall oral hygiene and exist-ing tissue in the mouth can be preserved. Some disadvantages of serial extraction are that it cannot be universally applied to all patients, treat-ment is spread out over many years, patient coopera-tion is needed, and there is a tendency to develop a tongue thrust. Contraindications noted include congenital absence of teeth providing space, mild to moderate crowding, deep or open bites, cleft lip and palate, a spaced denti-tion, disproportion between arc length and tooth mate-rial, and midline diastema. In the case shown here, (Fig. 9) we began nonextrac-tion therapy on the older brother with heavy therapy using the MDA appliance. I then used techniques taught by Dr. Gerety with distalization of the upper arch and potentially some limited mandibular advancement due to the elastics and eventually spring usage. The patient was not very compliant with elastics. After initial expan-sion with wires was completed, the MDA was not distal-izing very quickly or very well, and hygiene continued Fig. 10 to deteriorate. Brackets were soon coming off due to plaque accumulation and springs were tied in to aid in compliance with the MDA. After over 24 months of treatment, the mother and son were “done” with treat-ment and requested the remaining brackets and orthodontic appliances be removed. (Fig. 10) At the time we were approaching two years with his care, the boy’s sister came in with a mixed dentition and similar initial crowding, which can be seen in Fig. 11. Normally, I am averse to unnecessary tooth www.orthodontics.com Summer 2018 17
Journal of the American Orthodontic Society Summer 2018/Buyer's Guide: Page 17