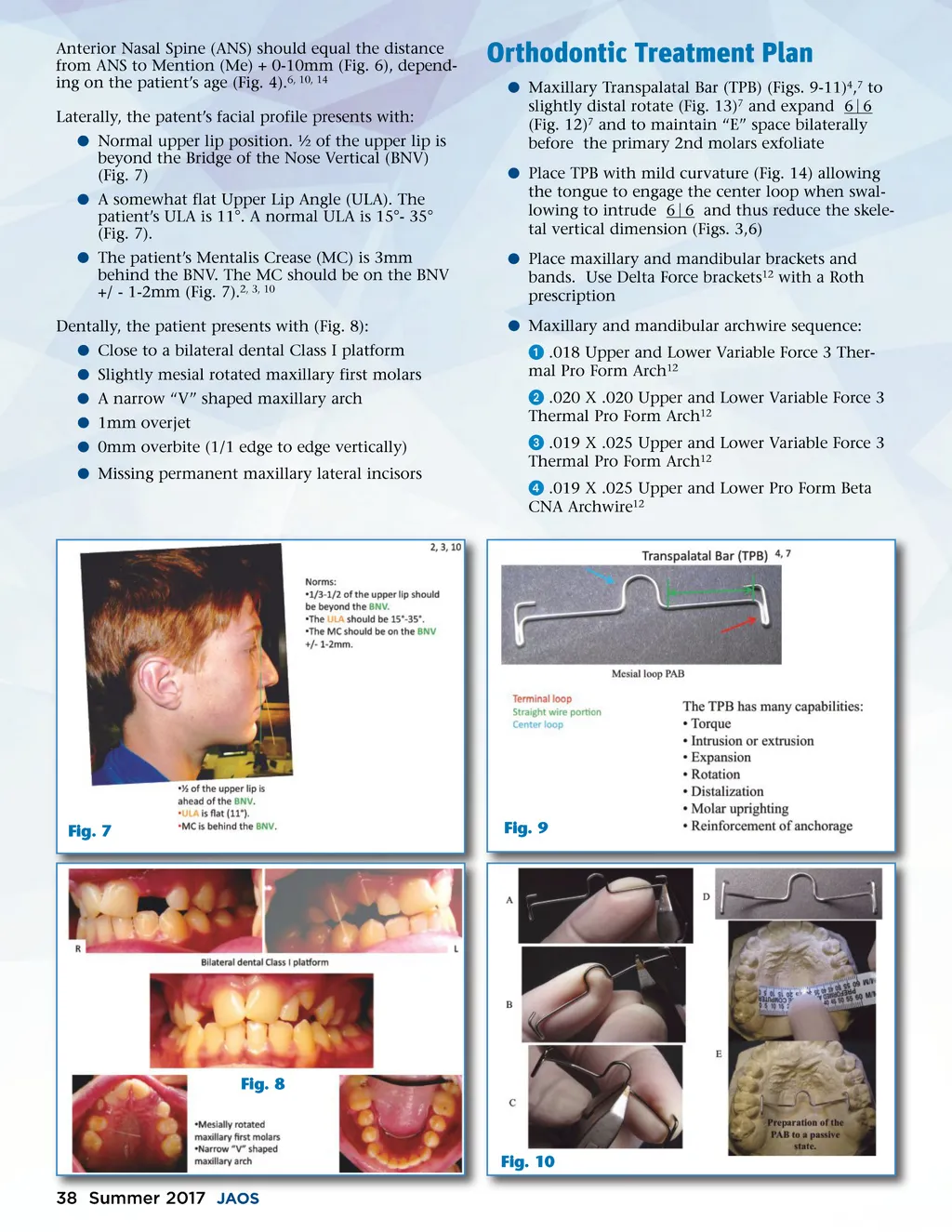
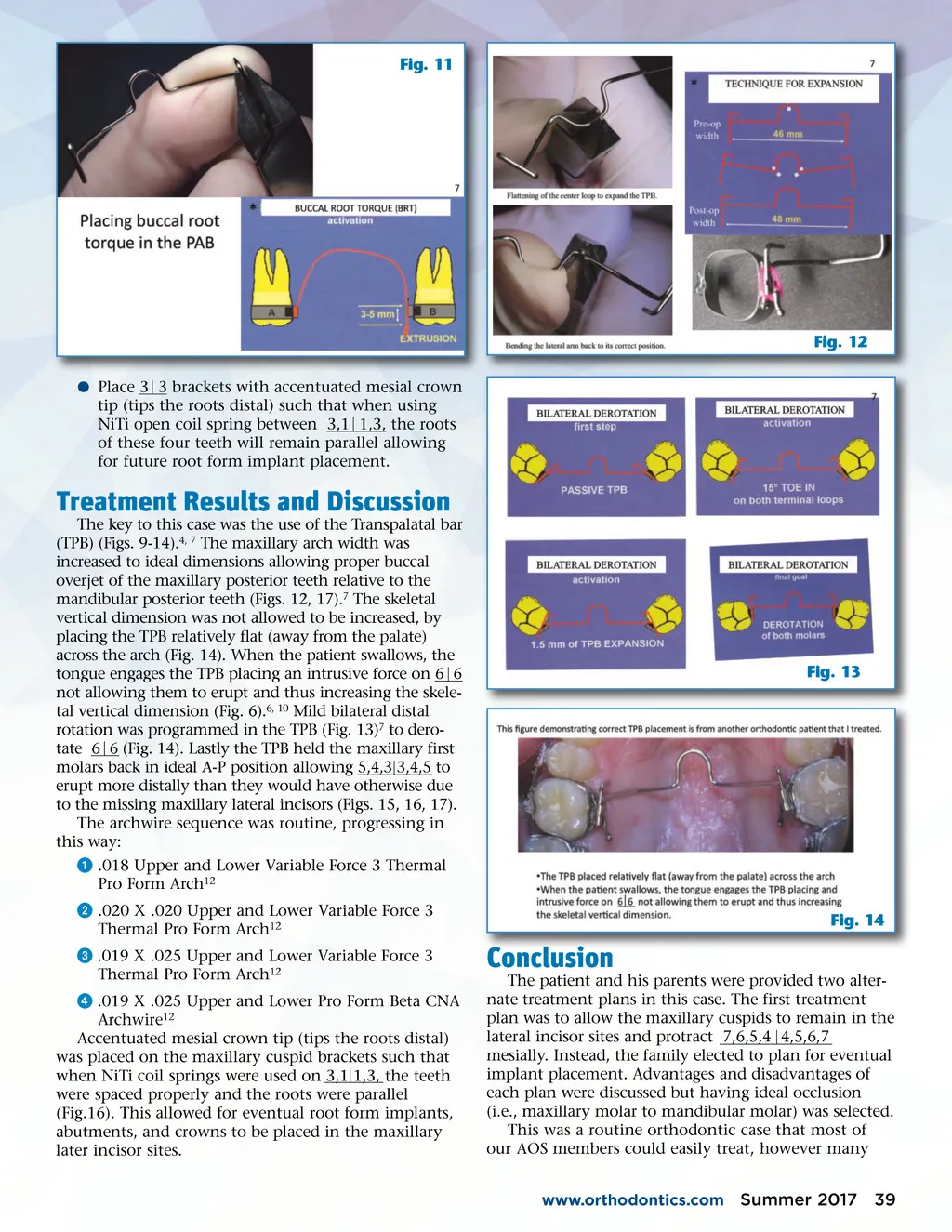
Fig. 11 Fig. 12 b Place 3 3 brackets with accentuated mesial crown tip (tips the roots distal) such that when using NiTi open coil spring between 3,1 1,3, the roots of these four teeth will remain parallel allowing for future root form implant placement. Treatment Results and Discussion The key to this case was the use of the Transpalatal bar (TPB) (Figs. 9-14). 4, 7 The maxillary arch width was increased to ideal dimensions allowing proper buccal overjet of the maxillary posterior teeth relative to the mandibular posterior teeth (Figs. 12, 17). 7 The skeletal vertical dimension was not allowed to be increased, by placing the TPB relatively flat (away from the palate) across the arch (Fig. 14). When the patient swallows, the tongue engages the TPB placing an intrusive force on 6 6 not allowing them to erupt and thus increasing the skele-tal vertical dimension (Fig. 6). 6, 10 Mild bilateral distal rotation was programmed in the TPB (Fig. 13) 7 to dero-tate 6 6 (Fig. 14). Lastly the TPB held the maxillary first molars back in ideal A-P position allowing 5,4,3 3,4,5 to erupt more distally than they would have otherwise due to the missing maxillary lateral incisors (Figs. 15, 16, 17). The archwire sequence was routine, progressing in this way: ᕡ .018 Upper and Lower Variable Force 3 Thermal Pro Form Arch 12 ᕢ .020 X .020 Upper and Lower Variable Force 3 Thermal Pro Form Arch 12 ᕣ .019 X .025 Upper and Lower Variable Force 3 Thermal Pro Form Arch 12 ᕤ .019 X .025 Upper and Lower Pro Form Beta CNA Archwire 12 Accentuated mesial crown tip (tips the roots distal) was placed on the maxillary cuspid brackets such that when NiTi coil springs were used on 3,1 1,3, the teeth were spaced properly and the roots were parallel (Fig.16). This allowed for eventual root form implants, abutments, and crowns to be placed in the maxillary later incisor sites. Fig. 13 Fig. 14 Conclusion The patient and his parents were provided two alter-nate treatment plans in this case. The first treatment plan was to allow the maxillary cuspids to remain in the lateral incisor sites and protract 7,6,5,4 4,5,6,7 mesially. Instead, the family elected to plan for eventual implant placement. Advantages and disadvantages of each plan were discussed but having ideal occlusion (i.e., maxillary molar to mandibular molar) was selected. This was a routine orthodontic case that most of our AOS members could easily treat, however many www.orthodontics.com Summer 2017 39
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 39