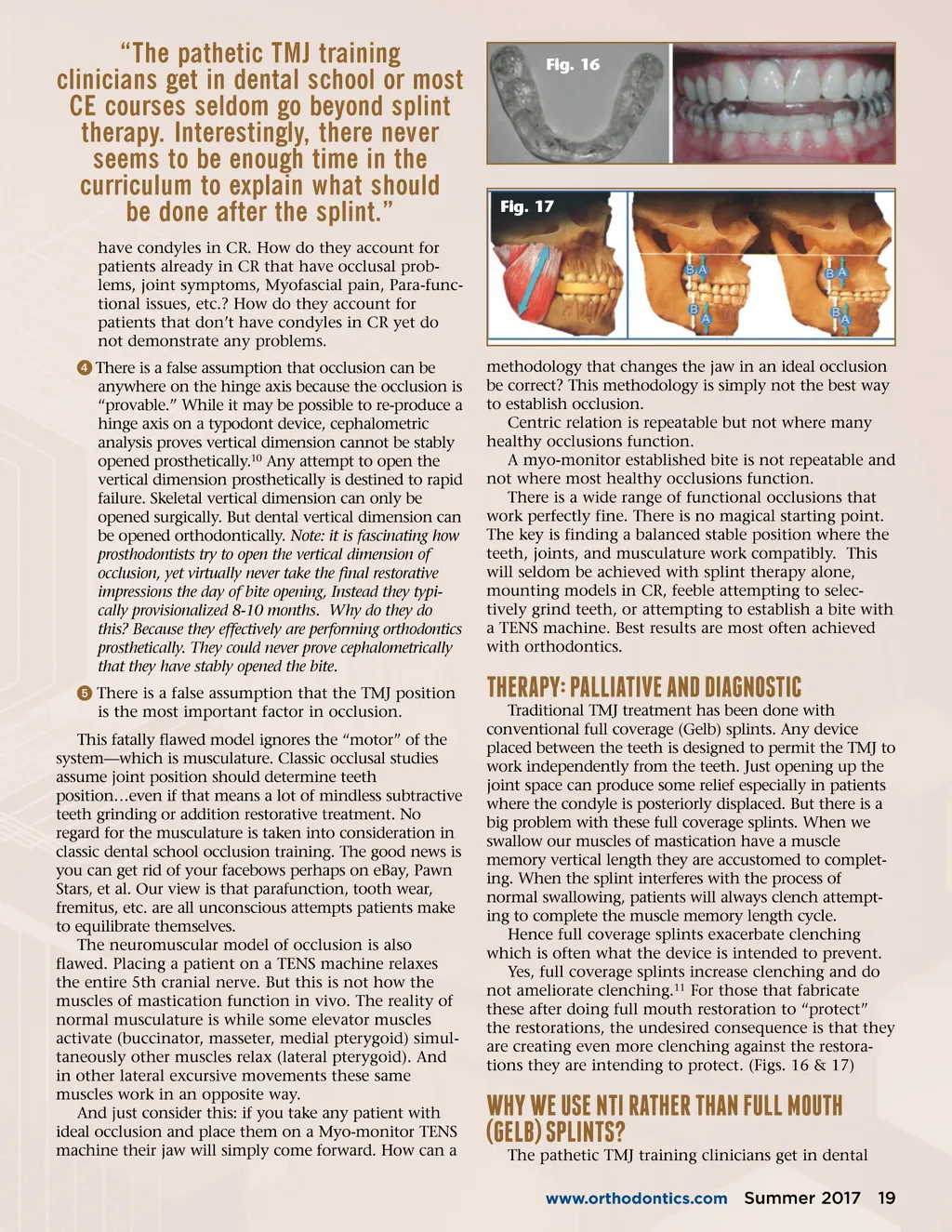
“The pathetic TMJ training clinicians get in dental school or most CE courses seldom go beyond splint therapy. Interestingly, there never seems to be enough time in the curriculum to explain what should be done after the splint.” have condyles in CR. How do they account for patients already in CR that have occlusal prob-lems, joint symptoms, Myofascial pain, Para-func-tional issues, etc.? How do they account for patients that don’t have condyles in CR yet do not demonstrate any problems. ᕤ There is a false assumption that occlusion can be anywhere on the hinge axis because the occlusion is “provable.” While it may be possible to re-produce a hinge axis on a typodont device, cephalometric analysis proves vertical dimension cannot be stably opened prosthetically. 10 Any attempt to open the vertical dimension prosthetically is destined to rapid failure. Skeletal vertical dimension can only be opened surgically. But dental vertical dimension can be opened orthodontically. Note: it is fascinating how prosthodontists try to open the vertical dimension of occlusion, yet virtually never take the final restorative impressions the day of bite opening, Instead they typi-cally provisionalized 8-10 months. Why do they do this? Because they effectively are performing orthodontics prosthetically. They could never prove cephalometrically that they have stably opened the bite. ᕥ There is a false assumption that the TMJ position is the most important factor in occlusion. This fatally flawed model ignores the “motor” of the system—which is musculature. Classic occlusal studies assume joint position should determine teeth position…even if that means a lot of mindless subtractive teeth grinding or addition restorative treatment. No regard for the musculature is taken into consideration in classic dental school occlusion training. The good news is you can get rid of your facebows perhaps on eBay, Pawn Stars, et al. Our view is that parafunction, tooth wear, fremitus, etc. are all unconscious attempts patients make to equilibrate themselves. The neuromuscular model of occlusion is also flawed. Placing a patient on a TENS machine relaxes the entire 5th cranial nerve. But this is not how the muscles of mastication function in vivo. The reality of normal musculature is while some elevator muscles activate (buccinator, masseter, medial pterygoid) simul-taneously other muscles relax (lateral pterygoid). And in other lateral excursive movements these same muscles work in an opposite way. And just consider this: if you take any patient with ideal occlusion and place them on a Myo-monitor TENS machine their jaw will simply come forward. How can a Fig. 16 Fig. 17 methodology that changes the jaw in an ideal occlusion be correct? This methodology is simply not the best way to establish occlusion. Centric relation is repeatable but not where many healthy occlusions function. A myo-monitor established bite is not repeatable and not where most healthy occlusions function. There is a wide range of functional occlusions that work perfectly fine. There is no magical starting point. The key is finding a balanced stable position where the teeth, joints, and musculature work compatibly. This will seldom be achieved with splint therapy alone, mounting models in CR, feeble attempting to selec-tively grind teeth, or attempting to establish a bite with a TENS machine. Best results are most often achieved with orthodontics. Traditional TMJ treatment has been done with conventional full coverage (Gelb) splints. Any device placed between the teeth is designed to permit the TMJ to work independently from the teeth. Just opening up the joint space can produce some relief especially in patients where the condyle is posteriorly displaced. But there is a big problem with these full coverage splints. When we swallow our muscles of mastication have a muscle memory vertical length they are accustomed to complet-ing. When the splint interferes with the process of normal swallowing, patients will always clench attempt-ing to complete the muscle memory length cycle. Hence full coverage splints exacerbate clenching which is often what the device is intended to prevent. Yes, full coverage splints increase clenching and do not ameliorate clenching. 11 For those that fabricate these after doing full mouth restoration to “protect” the restorations, the undesired consequence is that they are creating even more clenching against the restora-tions they are intending to protect. (Figs. 16 & 17) ThERApy: pAlliATivE AND DiAgNosTic Why WE usE NTi RAThER ThAN full MouTh (gElb) spliNTs? www.orthodontics.com The pathetic TMJ training clinicians get in dental Summer 2017 19
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 19