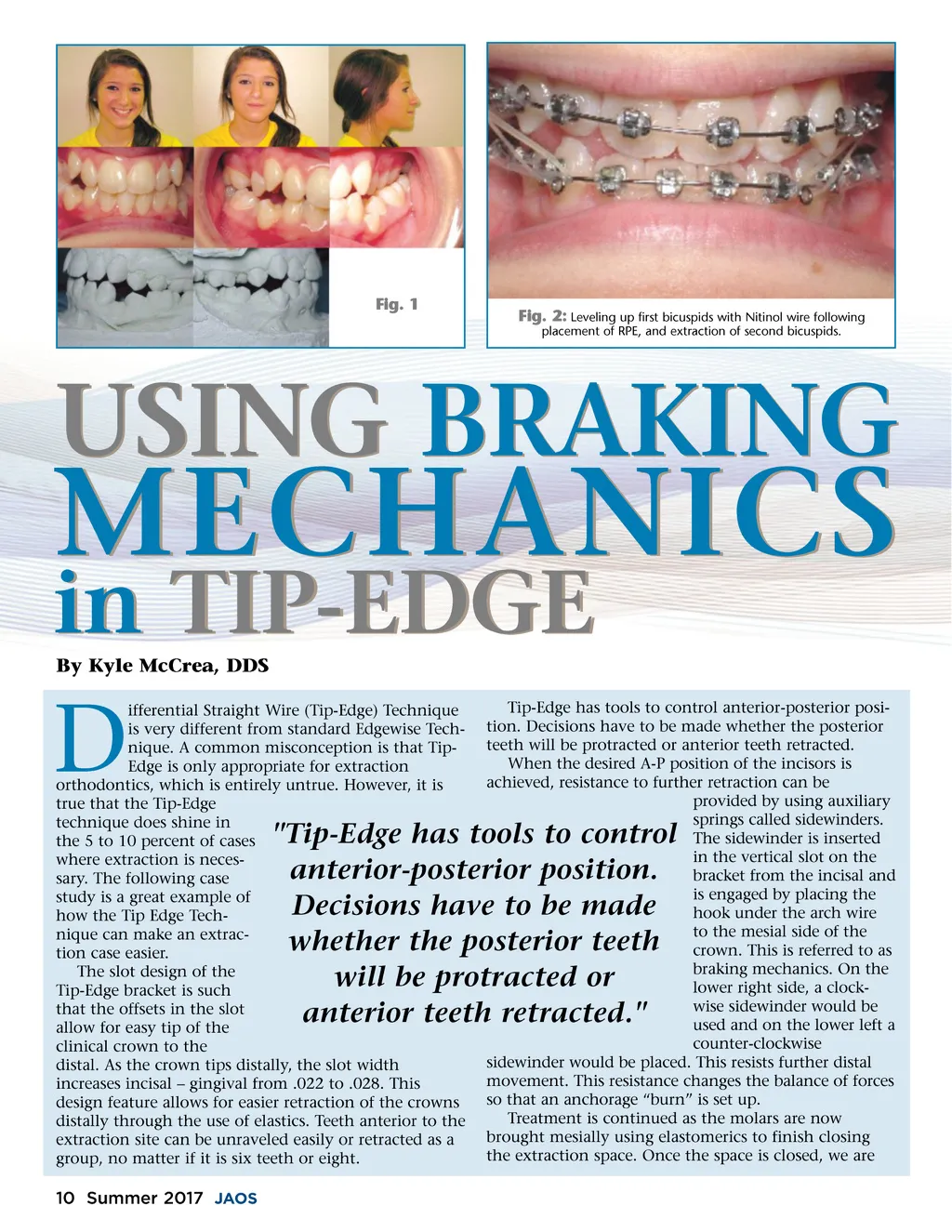
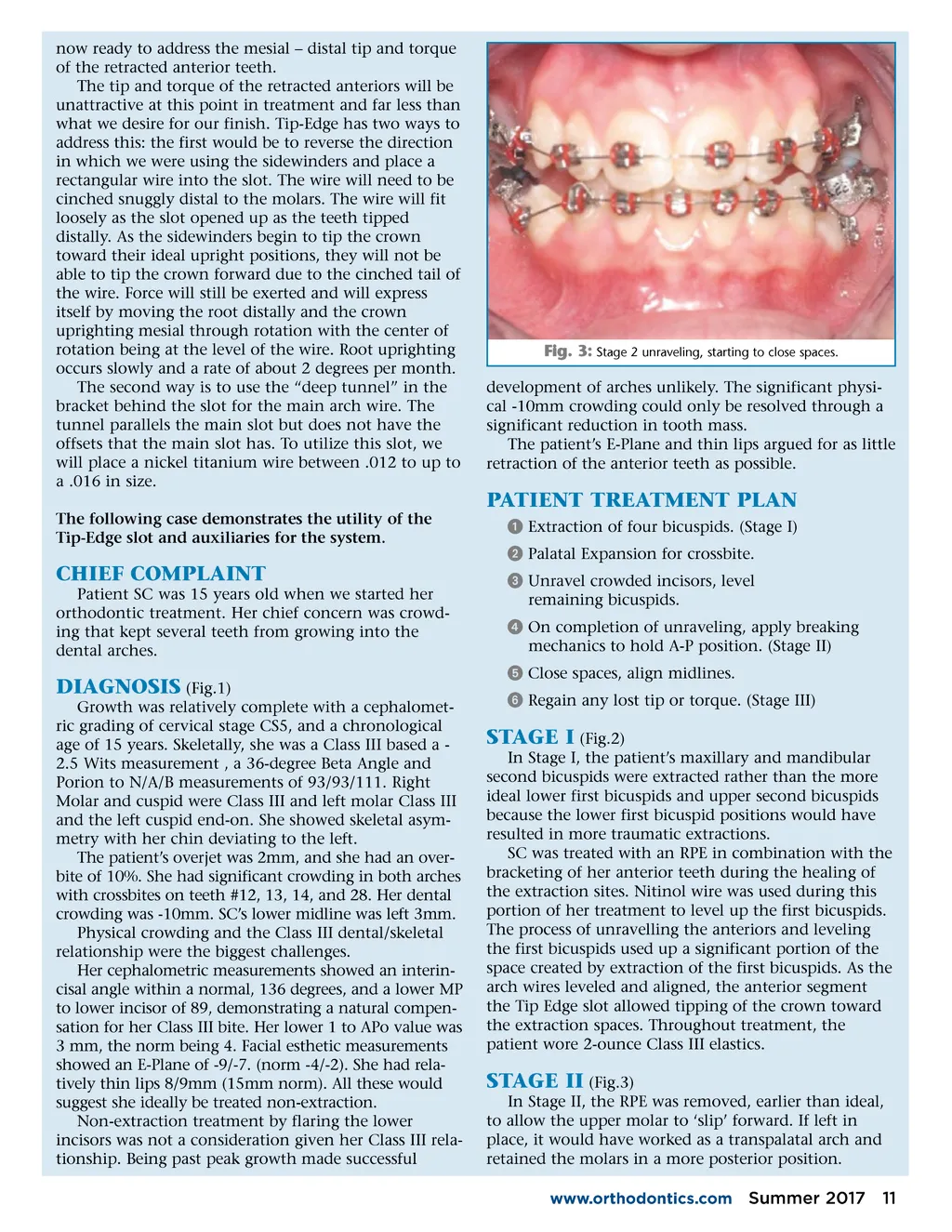
now ready to address the mesial – distal tip and torque of the retracted anterior teeth. The tip and torque of the retracted anteriors will be unattractive at this point in treatment and far less than what we desire for our finish. Tip-Edge has two ways to address this: the first would be to reverse the direction in which we were using the sidewinders and place a rectangular wire into the slot. The wire will need to be cinched snuggly distal to the molars. The wire will fit loosely as the slot opened up as the teeth tipped distally. As the sidewinders begin to tip the crown toward their ideal upright positions, they will not be able to tip the crown forward due to the cinched tail of the wire. Force will still be exerted and will express itself by moving the root distally and the crown uprighting mesial through rotation with the center of rotation being at the level of the wire. Root uprighting occurs slowly and a rate of about 2 degrees per month. The second way is to use the “deep tunnel” in the bracket behind the slot for the main arch wire. The tunnel parallels the main slot but does not have the offsets that the main slot has. To utilize this slot, we will place a nickel titanium wire between .012 to up to a .016 in size. The following case demonstrates the utility of the Tip-Edge slot and auxiliaries for the system. Fig. 3: Stage 2 unraveling, starting to close spaces. development of arches unlikely. The significant physi-cal -10mm crowding could only be resolved through a significant reduction in tooth mass. The patient’s E-Plane and thin lips argued for as little retraction of the anterior teeth as possible. PATIENT TREATMENT PLAN ᕡ Extraction of four bicuspids. (Stage I) ᕢ Palatal Expansion for crossbite. ᕣ Unravel crowded incisors, level remaining bicuspids. ᕤ On completion of unraveling, apply breaking mechanics to hold A-P position. (Stage II) ᕥ Close spaces, align midlines. ᕦ Regain any lost tip or torque. (Stage III) CHIEF COMPLAINT Patient SC was 15 years old when we started her orthodontic treatment. Her chief concern was crowd-ing that kept several teeth from growing into the dental arches. DIAGNOSIS (Fig.1) Growth was relatively complete with a cephalomet-ric grading of cervical stage CS5, and a chronological age of 15 years. Skeletally, she was a Class III based a -2.5 Wits measurement , a 36-degree Beta Angle and Porion to N/A/B measurements of 93/93/111. Right Molar and cuspid were Class III and left molar Class III and the left cuspid end-on. She showed skeletal asym-metry with her chin deviating to the left. The patient’s overjet was 2mm, and she had an over-bite of 10%. She had significant crowding in both arches with crossbites on teeth #12, 13, 14, and 28. Her dental crowding was -10mm. SC’s lower midline was left 3mm. Physical crowding and the Class III dental/skeletal relationship were the biggest challenges. Her cephalometric measurements showed an interin-cisal angle within a normal, 136 degrees, and a lower MP to lower incisor of 89, demonstrating a natural compen-sation for her Class III bite. Her lower 1 to APo value was 3 mm, the norm being 4. Facial esthetic measurements showed an E-Plane of -9/-7. (norm -4/-2). She had rela-tively thin lips 8/9mm (15mm norm). All these would suggest she ideally be treated non-extraction. Non-extraction treatment by flaring the lower incisors was not a consideration given her Class III rela-tionship. Being past peak growth made successful STAGE I (Fig.2) In Stage I, the patient’s maxillary and mandibular second bicuspids were extracted rather than the more ideal lower first bicuspids and upper second bicuspids because the lower first bicuspid positions would have resulted in more traumatic extractions. SC was treated with an RPE in combination with the bracketing of her anterior teeth during the healing of the extraction sites. Nitinol wire was used during this portion of her treatment to level up the first bicuspids. The process of unravelling the anteriors and leveling the first bicuspids used up a significant portion of the space created by extraction of the first bicuspids. As the arch wires leveled and aligned, the anterior segment the Tip Edge slot allowed tipping of the crown toward the extraction spaces. Throughout treatment, the patient wore 2-ounce Class III elastics. STAGE II (Fig.3) In Stage II, the RPE was removed, earlier than ideal, to allow the upper molar to ‘slip’ forward. If left in place, it would have worked as a transpalatal arch and retained the molars in a more posterior position. www.orthodontics.com Summer 2017 11
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 11