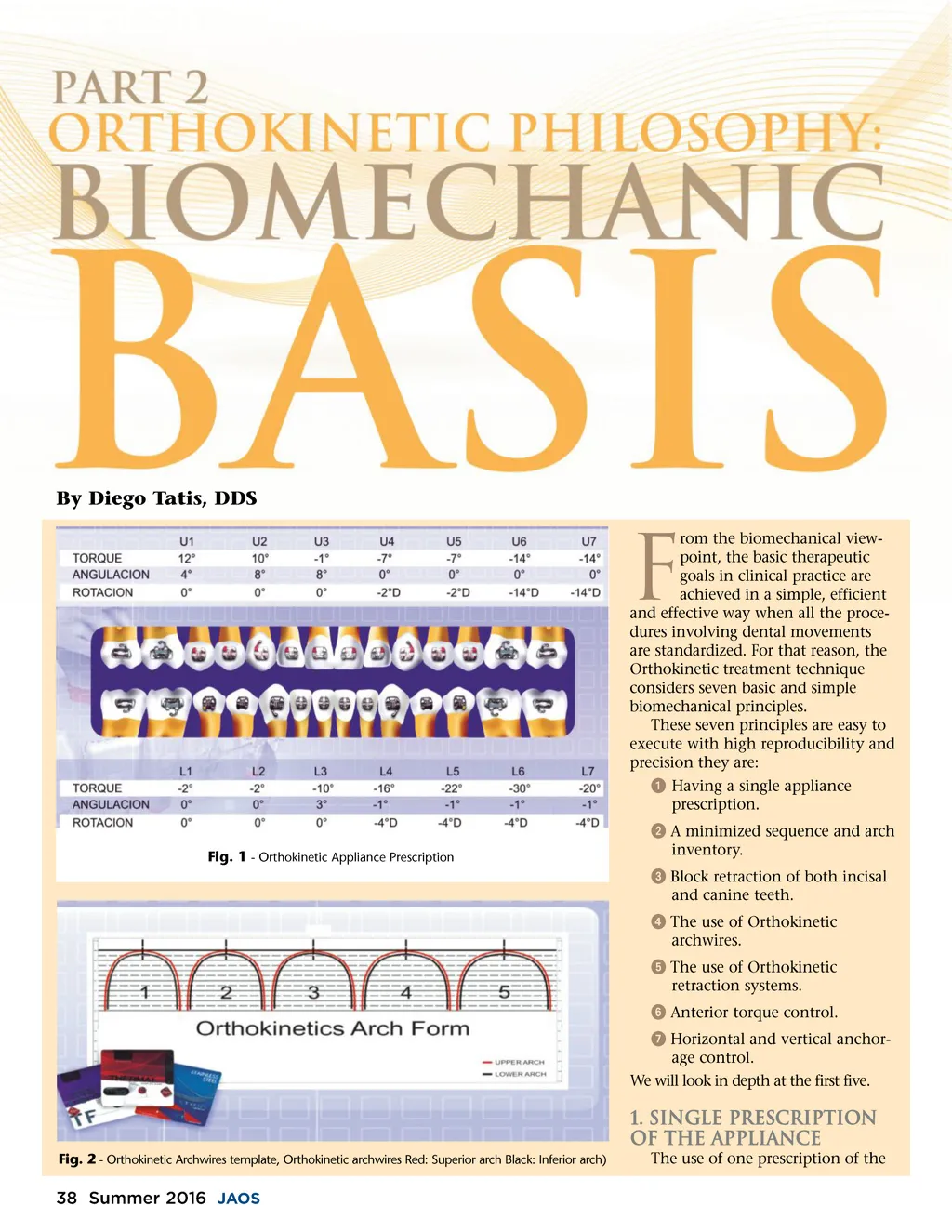
appliance that is adjustable to differ-ent clinical cases, such as cases with or without extractions, or with differ-ent anchorage requirements or for different patient biotypes. This reduces the inventory of appliances and standardizes the entire clinical and administrative processes. (Fig. 1) 2. Minimized Sequence and Arch Inventory The number of wires used during Orthokinetic treatment has been reduced to three. The initial archwire is an Alignment archwire. A heat-acti-vated nitinol 0.016-gauge archwire is used. In severe crowding cases, we use auxiliary systems to obtain space to attach these teeth with severs crowding or the initial smaller gauge archwire to establish space to allow the initiation of a 0.016 wire to the bracketed teeth. The second arch-wire used is a transition archwire. This archwire is a heat-activated nitinol 0.019 x 0.025 gauge wire; it prepares the slots for the working stage and the third arch-wire. This third Orthokinetic archwire is the final archwire and it is involved with case finalization and finishing. We can use either a 0.019 x 0.025 gauge stainless steel archwire or a 0.021 x 0.025 gauge stainless steel archwire in this working stage. The size and shape of the arch-wires used in the Orthokinetics mechanics come in templates marked with numbers 1 through 5 according to the increasing size. The author's research has found that five archwires best represent the size and shape of the arch. The template is printed in red for the upper arch and black for the lower arch, with the respective midline marked on each. The hori-zontal line at the base marks the guide and posterior symmetry of the arch and the superior parallel marks the anterior limit of the arch. In the lateral part, there are two auxiliary rulers to measure the archwire length according to the patient s dental arch size and to make counting easier outside the mouth rather than inside, which can be more difficult and take more chair time. The size of the arch is selected from the patient’s lower Fig. 3 -Intraoral photographs showing the sequence of block retraction in an extraction case. model, taking into account the ante-rior outline of the arch and the transversal posterior diameter from the last molar present to the level of the alveolar ridge. The shape and size of the arch must be selected for the patient at the beginning of the treatment, and during the mechanical sequence these numbers are duly observed to the arch confection. (Fig. 2) rior segment. (Fig. 3) 4. Use of Orthokinetic Archwire Orthokinetic archwire (abbreviated O.K.) are the archwires used to close spaces with sliding mechanics, during block retraction of the anterior segment from canine to canine or with mesial movement of the poste-rior segment (loss of anchorage). These wires are made of 0.019 x 0.025 stainless steel gauged archwire or 0.021 x 0.025 gauge stainless steel archwire and each has hooks adapted to the distal part of the canine teeth, to allow the retraction system to be engaged for space closure biomechan-ics (Fig. 4). The O.K. archwire hook is placed in the extraction space, making it different from the biomechanical wires. This is done because biome-chanical laboratory tests and its use over many years have shown there are clinical advantages. Through the history of orthodon-tics, most techniques and mechanics have considered the movement in the dental arch; both sagittal and trans-verse, as one structural unit and therefore they generate undesirable force vectors that ultimately produce reactions that complicate and prolonged the treatment and compro-3. Block Retraction of Incisal and Canine Teeth For cases with or without extrac-tions (when space closure is required), the retraction of anterior teeth is performed in block, from canine to canine. The block retrac-tion has some functional, esthetic and administrative advantages compared to the mechanics of first retracting the canine and then the incisal teeth. The first advantage is the reduc-tion in treatment time and cost. The second is a functional advantage, as in cases involving the extraction of four first premolar teeth. After the leveling and alignment phase, the patient is in a Class I canine relation-ship. Before retraction, begins the canine is both superior and inferior to the anterior segment, which allows us to have canine function during the entire whole space closuring stage. This protects the occluso-masticatory system during mandibular excursions. The third advantage is esthetic. As the block retraction of the anterior segment avoids the presence of any residual edentulous spaces in the ante-rior section for prolonged periods. And, finally, the changes in soft tissues that result from the retraction of anterior teeth are rapidly obtained with the block retraction of the ante-Fig. 4 -Orthokinetic archwire adapted with the hook distal to the canine bracket (A) and the retraction system in place (B) to close the space. www.orthodontics.com Summer 2016 39
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 39