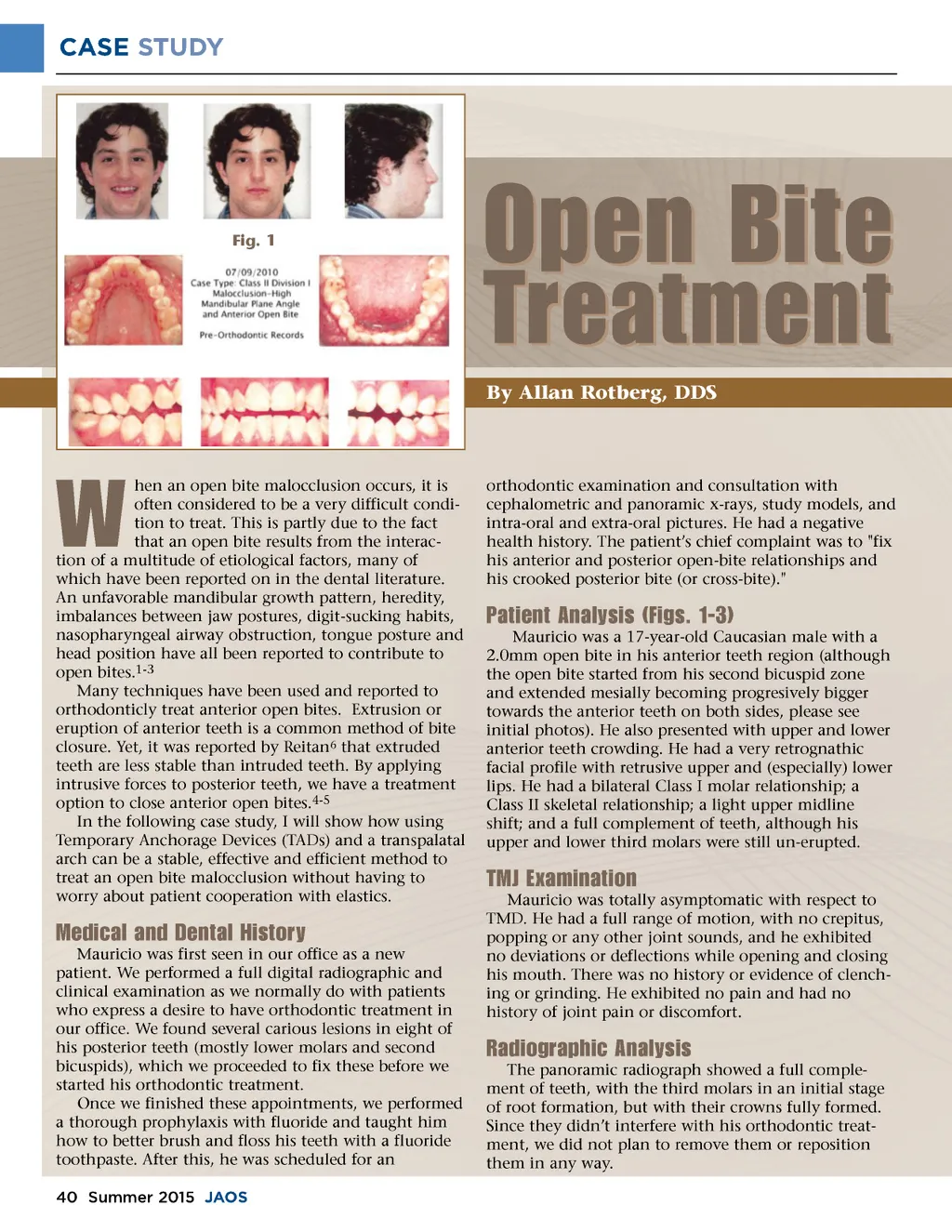
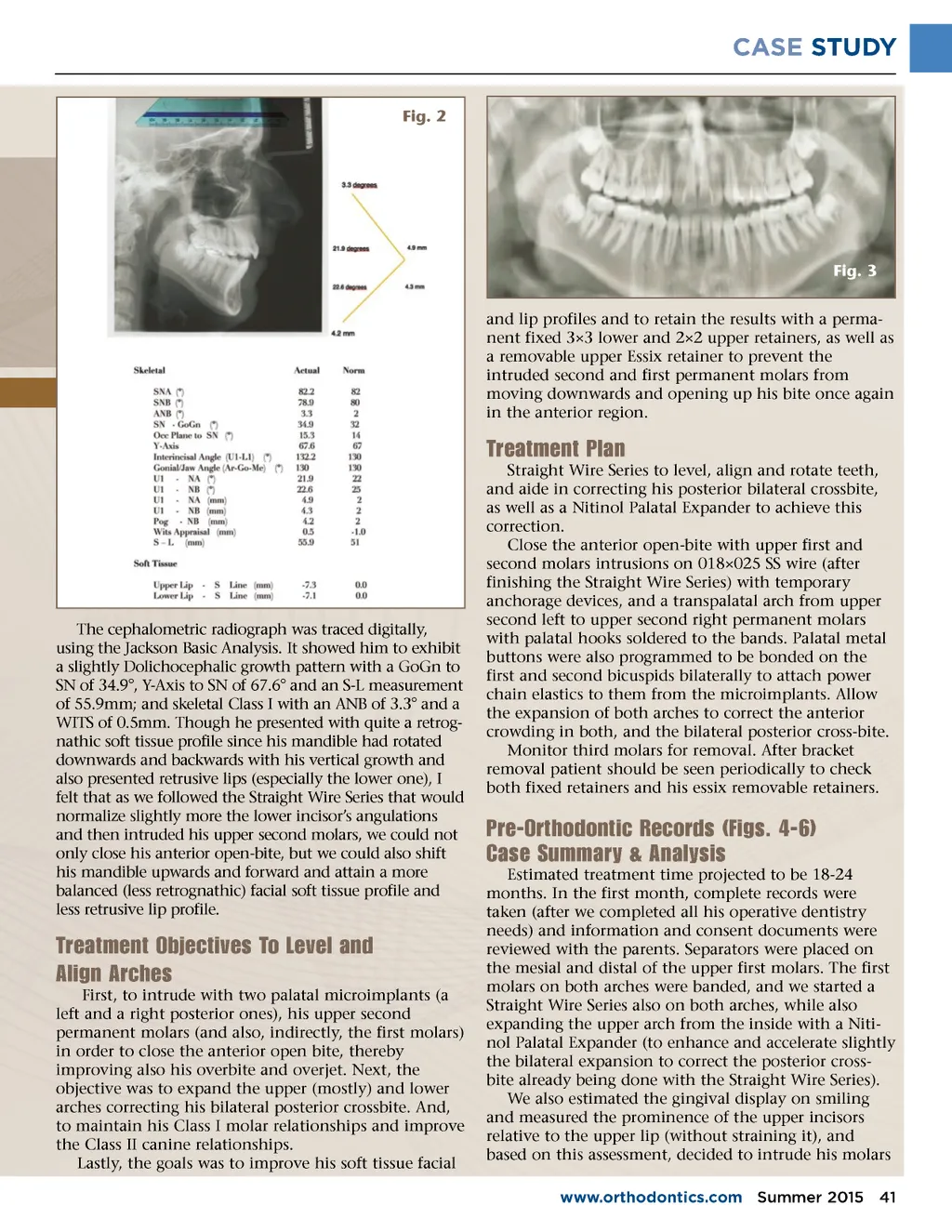
CASE STUDY Fig. 2 Fig. 3 and lip profiles and to retain the results with a perma-nent fixed 3×3 lower and 2×2 upper retainers, as well as a removable upper Essix retainer to prevent the intruded second and first permanent molars from moving downwards and opening up his bite once again in the anterior region. Treatment Plan Straight Wire Series to level, align and rotate teeth, and aide in correcting his posterior bilateral crossbite, as well as a Nitinol Palatal Expander to achieve this correction. Close the anterior open-bite with upper first and second molars intrusions on 018×025 SS wire (after finishing the Straight Wire Series) with temporary anchorage devices, and a transpalatal arch from upper second left to upper second right permanent molars with palatal hooks soldered to the bands. Palatal metal buttons were also programmed to be bonded on the first and second bicuspids bilaterally to attach power chain elastics to them from the microimplants. Allow the expansion of both arches to correct the anterior crowding in both, and the bilateral posterior cross-bite. Monitor third molars for removal. After bracket removal patient should be seen periodically to check both fixed retainers and his essix removable retainers. The cephalometric radiograph was traced digitally, using the Jackson Basic Analysis. It showed him to exhibit a slightly Dolichocephalic growth pattern with a GoGn to SN of 34.9°, Y-Axis to SN of 67.6° and an S-L measurement of 55.9mm; and skeletal Class I with an ANB of 3.3° and a WITS of 0.5mm. Though he presented with quite a retrog-nathic soft tissue profile since his mandible had rotated downwards and backwards with his vertical growth and also presented retrusive lips (especially the lower one), I felt that as we followed the Straight Wire Series that would normalize slightly more the lower incisor’s angulations and then intruded his upper second molars, we could not only close his anterior open-bite, but we could also shift his mandible upwards and forward and attain a more balanced (less retrognathic) facial soft tissue profile and less retrusive lip profile. Pre-Orthodontic Records (Figs. 4-6) Case Summary & Analysis Estimated treatment time projected to be 18-24 months. In the first month, complete records were taken (after we completed all his operative dentistry needs) and information and consent documents were reviewed with the parents. Separators were placed on the mesial and distal of the upper first molars. The first molars on both arches were banded, and we started a Straight Wire Series also on both arches, while also expanding the upper arch from the inside with a Niti-nol Palatal Expander (to enhance and accelerate slightly the bilateral expansion to correct the posterior cross-bite already being done with the Straight Wire Series). We also estimated the gingival display on smiling and measured the prominence of the upper incisors relative to the upper lip (without straining it), and based on this assessment, decided to intrude his molars www.orthodontics.com Summer 2015 41 Treatment Objectives To Level and Align Arches First, to intrude with two palatal microimplants (a left and a right posterior ones), his upper second permanent molars (and also, indirectly, the first molars) in order to close the anterior open bite, thereby improving also his overbite and overjet. Next, the objective was to expand the upper (mostly) and lower arches correcting his bilateral posterior crossbite. And, to maintain his Class I molar relationships and improve the Class II canine relationships. Lastly, the goals was to improve his soft tissue facial
Journal of the American Orthodontic Society Summer 2015-Buyer's Guide: Page 41