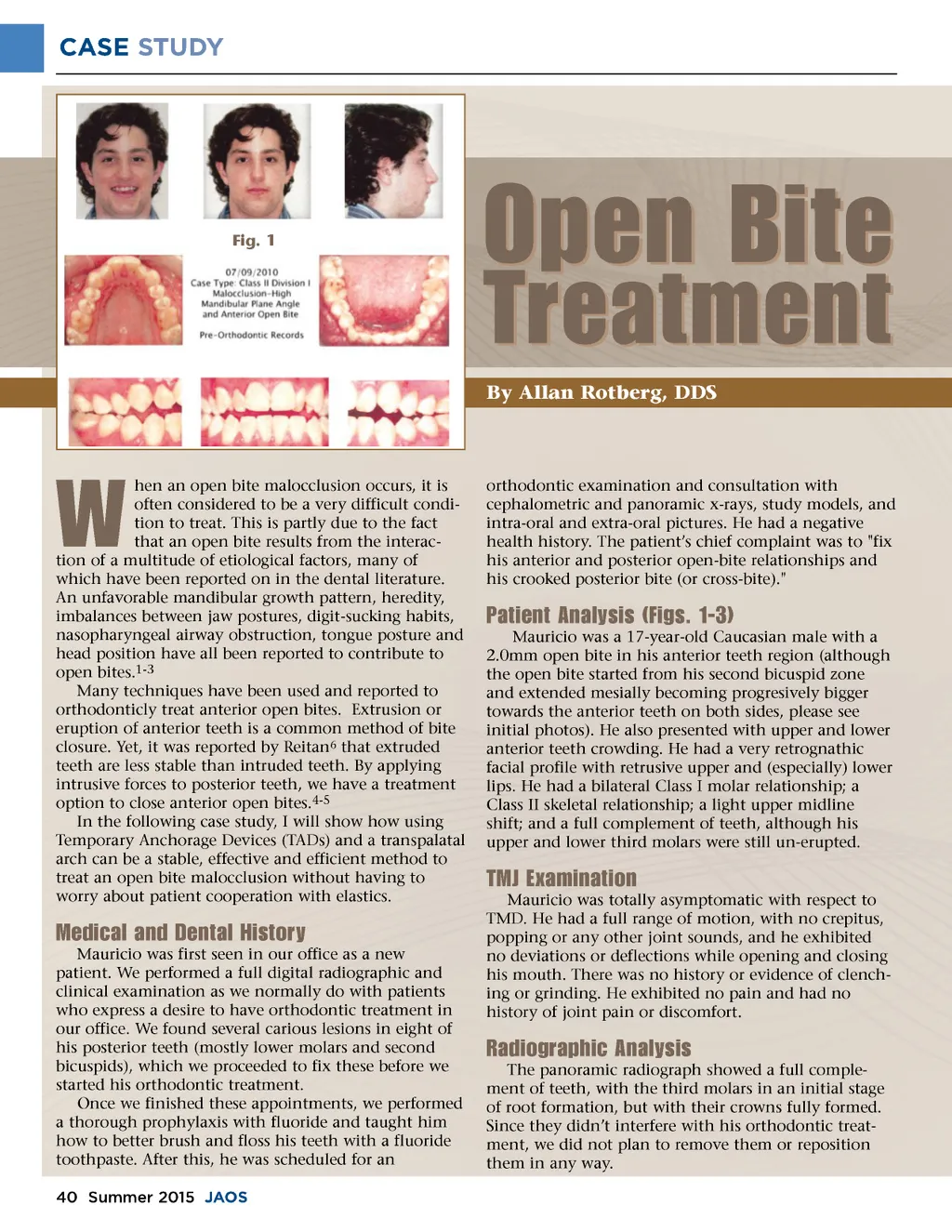
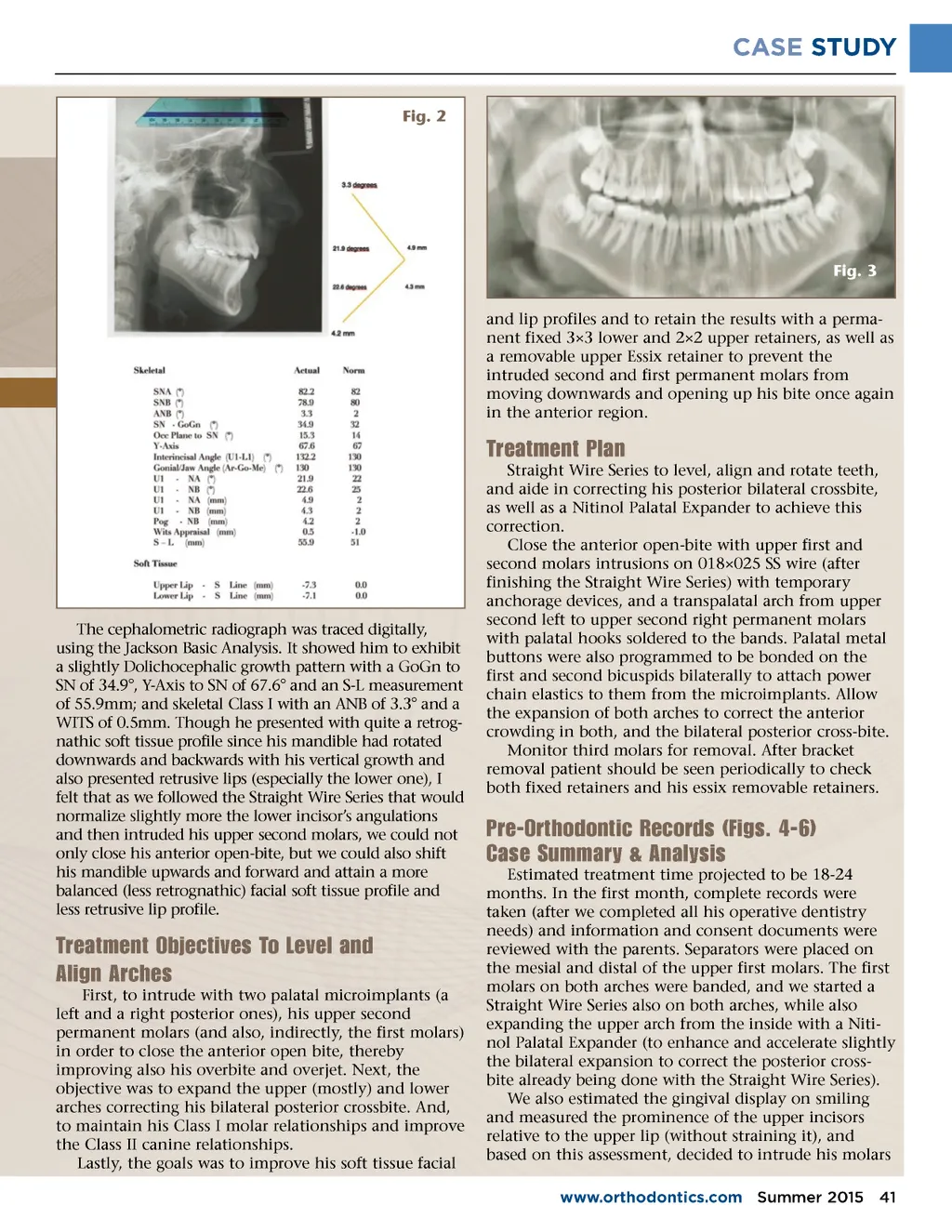
CASE STUDY Fig. 1 Open Bite Treatment By Allan Rotberg, DDS orthodontic examination and consultation with cephalometric and panoramic x-rays, study models, and intra-oral and extra-oral pictures. He had a negative health history. The patient’s chief complaint was to "fix his anterior and posterior open-bite relationships and his crooked posterior bite (or cross-bite)." W hen an open bite malocclusion occurs, it is often considered to be a very difficult condi-tion to treat. This is partly due to the fact that an open bite results from the interac-tion of a multitude of etiological factors, many of which have been reported on in the dental literature. An unfavorable mandibular growth pattern, heredity, imbalances between jaw postures, digit-sucking habits, nasopharyngeal airway obstruction, tongue posture and head position have all been reported to contribute to open bites. 1-3 Many techniques have been used and reported to orthodonticly treat anterior open bites. Extrusion or eruption of anterior teeth is a common method of bite closure. Yet, it was reported by Reitan 6 that extruded teeth are less stable than intruded teeth. By applying intrusive forces to posterior teeth, we have a treatment option to close anterior open bites. 4-5 In the following case study, I will show how using Temporary Anchorage Devices (TADs) and a transpalatal arch can be a stable, effective and efficient method to treat an open bite malocclusion without having to worry about patient cooperation with elastics. Patient Analysis (Figs. 1-3) Mauricio was a 17-year-old Caucasian male with a 2.0mm open bite in his anterior teeth region (although the open bite started from his second bicuspid zone and extended mesially becoming progresively bigger towards the anterior teeth on both sides, please see initial photos). He also presented with upper and lower anterior teeth crowding. He had a very retrognathic facial profile with retrusive upper and (especially) lower lips. He had a bilateral Class I molar relationship; a Class II skeletal relationship; a light upper midline shift; and a full complement of teeth, although his upper and lower third molars were still un-erupted. TMJ Examination Mauricio was totally asymptomatic with respect to TMD. He had a full range of motion, with no crepitus, popping or any other joint sounds, and he exhibited no deviations or deflections while opening and closing his mouth. There was no history or evidence of clench-ing or grinding. He exhibited no pain and had no history of joint pain or discomfort. Medical and Dental History Mauricio was first seen in our office as a new patient. We performed a full digital radiographic and clinical examination as we normally do with patients who express a desire to have orthodontic treatment in our office. We found several carious lesions in eight of his posterior teeth (mostly lower molars and second bicuspids), which we proceeded to fix these before we started his orthodontic treatment. Once we finished these appointments, we performed a thorough prophylaxis with fluoride and taught him how to better brush and floss his teeth with a fluoride toothpaste. After this, he was scheduled for an 40 Summer 2015 JAOS Radiographic Analysis The panoramic radiograph showed a full comple-ment of teeth, with the third molars in an initial stage of root formation, but with their crowns fully formed. Since they didn’t interfere with his orthodontic treat-ment, we did not plan to remove them or reposition them in any way.
Journal of the American Orthodontic Society Summer 2015-Buyer's Guide: Page 40